Postmenopausal AUB: Rule out endometrial cancer first






When a postmenopausal woman presents with abnormal uterine bleeding, endometrial cancer is the biggest concern. But a host of other etiologies also are possible. The author reviews them and outlines a systematic approach to diagnosis.
Endometrial biopsy is another option for patients with postmenopausal AUB, though the American College of Obstetricians and Gynecologists (ACOG) does not recommend this method for screening asymptomatic menopausal women not on HRT.3 The evidence: Korhonen et al evaluated screening by endometrial biopsy in 2,964 peri- and post-menopausal women, ages 40 to 66 (mean age, 52), who were not on HRT. They identified 19 samples with simple endometrial hyperplasia without cytologic atypia (0.6%) and only 2 cases of well-differentiated adenocarcinoma of the endometrium (0.07%). The majority of the endometrial samples (68.7%) were atrophic, and approximately 25% were proliferative.4
Since the cost-effectiveness of endometrial biopsy and TVUS of the endometrium are comparable, the choice of modality rests with the physician. If TVUS is performed, an endometrial thickness of 4 mm or less is associated with endometrial cancer in about 0.6% of cases.5 If the endometrial thickness is greater than 4 mm, a sonohysterogram should be performed to determine whether the endometrium is symmetrically thickened. If it is, an endometrial biopsy also should be obtained. If an asymmetrical filling defect is found, hysteroscopy and directed biopsy are recommended (FIGURE 1). In women with continued bleeding after a negative initial evaluation, further testing with hysteroscopically directed biopsy is essential, since approximately 4% of these patients will have underlying pathology detected on subsequent evaluation.6
FIGURE 1 Initial management of postmenopausal bleeding
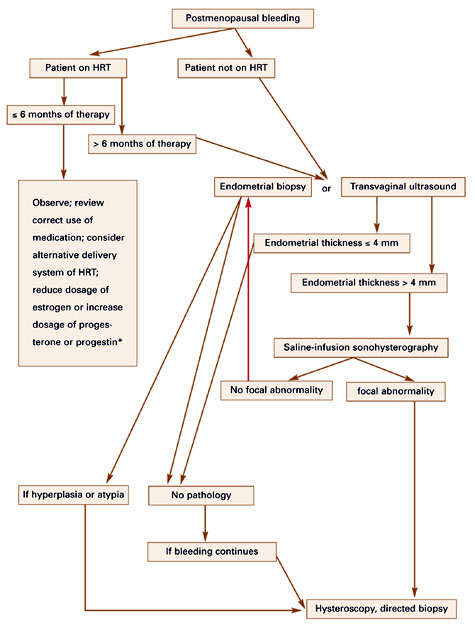
HRT = hormone replacement therapy
*Endometrial thickness acts as a surrogate marker for the combined biologic estrogenic and progestogenic effect on the endometrium.
Anatomic problems
In up to 30% of cases, postmenopausal bleeding is associated with an anatomic abnormality (TABLE 2).7 TVUS and saline-infusion sonohysterography are helpful in identifying these abnormalities. Uterine fibroids and adenomyomas generally are apparent on ultrasound. Uterine polyps may appear as a thickened endometrial stripe, but these and submucous myomas can be clearly identified as filling defects when a sonohysterography is performed.
Tamoxifen is associated with a two- to threefold increased risk of endometrial cancer in postmenopausal women.
A Pap smear should be obtained if the patient has not had 1 within the past year, although cervical disease is an uncommon cause of postmenopausal bleeding. Still, atypical endometrial cells occasionally are noted on a Pap smear. This should prompt an endometrial biopsy or other histologic examination.
TABLE 2
Anatomic causes of postmenopausal bleeding
| UTERUS | CERVIX | OVARY | VAGINA/VULVA |
|---|---|---|---|
| Submucosal fibroid | Cervical polyps | Estrogen-secreting tumor | Atrophic vaginitis |
| Endometrial polyp | Cervical erosion/cervicitis | Vaginal neoplasm | |
| Endometrial hyperplasia | Cervical cancer | Vulvar carcinoma | |
| Adenomyosis | |||
| Endometritis | |||
| Adenocarcinoma | |||
| Sarcoma |
Systemic conditions
Abnormalities of the hematologic system also must be considered as a possible cause of post menopausal bleeding (TABLE 3). On rare occasions, AUB will be the first sign of leukemia or a blood dyscrasia. By the menopausal years, a woman should know whether she has von Willebrand’s disease, factor IX deficiency, an inherited clotting disorder, or other disorders that may cause menorrhagia in premenopausal women but are unlikely to be the reason for postmenopausal bleeding. Overuse of anticoagulant medications such as aspirin, heparin, and warfarin—which are taken with greater frequency by patients in this age group—may contribute to post-menopausal bleeding, although this accounts for a minority of cases. Still, uterine bleeding that occurs in conjunction with these agents may unmask an underlying uterine problem. Thus, in this scenario, it is worthwhile to evaluate the endometrium with TVUS or saline-infusion sonohysterography.
TABLE 3
Nonanatomic causes of postmenopausal bleeding
| HRT USERS | NON-HRT USERS |
|---|---|
| Improper use of HRT | Atrophic endometrium |
| Poor absorption of HRT due to ulcerative colitis or Crohn’s disease | Endometrial polyp or neoplasm related to tamoxifen therapy |
| Drug interactions with hepatic enzyme inducers (SSRIs, phenytoin, barbiturates, griseofulvin) | |
| Coagulation defects:* | |
| Thrombocytopenia | |
| von Willebrand’s disease | |
| Leukemia | |
| Anticoagulant excess | |
| Inadequate progestational response at the endometrium | |
| HRT = hormone replacement therapy; SSRI = selective serotonin reuptake inhibitor | |
| *Uterine bleeding may occur in any women with these conditions, though it is more likely with HRT use. | |
Tamoxifen use
Tamoxifen therapy is associated with a two-to threefold increased risk of endometrial cancer in postmenopausal women.8 TVUS of patients on this therapy typically shows an increased endometrial thickness. Risk appears to increase with higher cumulative doses of tamoxifen and longer duration of treatment. For these reasons, uterine bleeding in women aking tamoxifen should be evaluated with saline-infusion sonohysterography. If the endometrium is symmetrically thickened, an endometrial biopsy should be performed. If an endometrial filling defect, such as a polyp, is identified, hysteroscopically directed biopsy is in order.
Postmenopausal bleeding and HRT
The occurrence of uterine bleeding or spotting after the initiation of HRT is not unusual. More than half of HRT users will have some spotting or bleeding at the beginning of therapy. Usually such bleeding is lighter than a menstrual period and lessens with time; after 6 months, it stops completely in most women.9 The dose and type of progestin used in the HRT regimen, as well as the length of time since menopause, also affect the occurrence of bleeding. Women more than 3 years beyond menopause when starting HRT have fewer episodes of bleeding and are more likely to be amenorrheic after 3 months of treatment than women who start HRT within 3 years of menopause.10