
Laparoscopic evaluation of the pelvis: refocusing on the basics






When a systematic approach is utilized, pelvic laparoscopy can aid clinicians in diagnosing a range of common conditions. Here, the author offers techniques for ensuring accurate findings, and reviews snapshots of various abnormalities.
Laparoscopic procedures. It may sometimes be appropriate to perform surgical therapy during a pelvic evaluation. For example, most ectopic pregnancies can be treated laparoscopically, as can many cases of endometriosis. It is desirable, however, to complete the pelvic examination before performing any subsequent procedures, including the removal of ovarian cysts, ovaries, fibroids, or the uterus, since blood and peritoneal trauma may make abnormal findings difficult to perceive.
FIGURE 1A Inner concentric circle
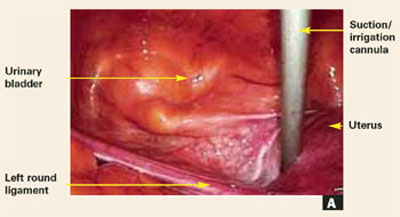
FIGURE 1B Inner concentric circle
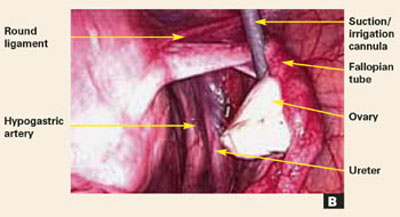
FIGURE 1C Inner concentric circle
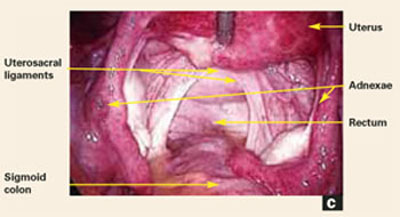
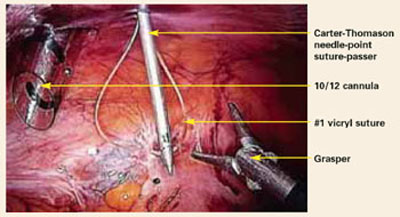
FIGURE 1D Inner concentric circle
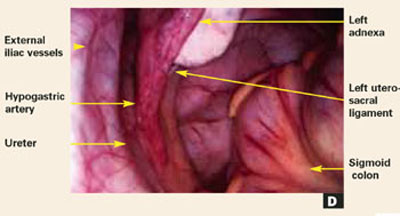
FIGURE 2A Outer concentric circle
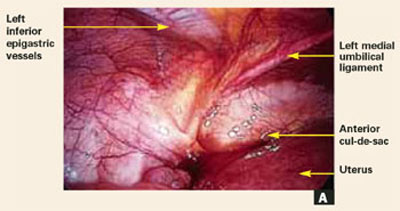
FIGURE 2B Outer concentric circle
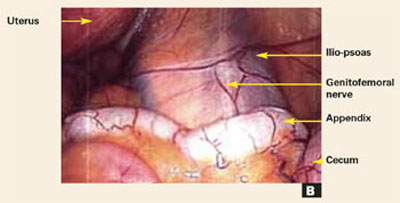
FIGURE 2C Outer concentric circle
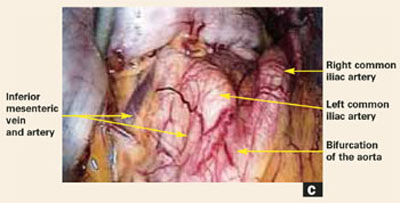
FIGURE 3
Avoiding complications
Laparoscopic complications can be minimized by using safe techniques during patient preparation, abdominal entry and exit, and while conducting operative procedures. Prior to some pelvic inspections, it may be necessary to lyse adhesions of the omentum or bowel to minimize injury to those organs and to get a better view of the pelvis. In these cases, use atraumatic forceps to achieve a better plane for dissection. Consider using ultrasonic shears to minimize thermal injury to the bowel.
In addition to closing the peritoneum and fascia at all sites greater than 5 mm, you can prevent trocar site hernias by avoiding extensive manipulation, carbon dioxide leakage during the course of surgery, and repeated replacement of the cannula, all of which can contribute to trocar site dilatation.
Trocar sites may be associated not only with hernias—which cause acute and severe symptoms requiring immediate intervention—but also with adhesions resulting in chronic pelvic pain.
When patients postoperatively complain of pain, nausea, and vomiting, and a mass is palpable at the trocar site, a port site hernia should be suspected. Plain abdominal x-rays usually indicate a partial small bowel obstruction. In such cases, promptly obtain a computed tomography (CT) scan, which will confirm the diagnosis. This condition can be managed laparoscopically if it is diagnosed early, but the operator must take extra care when making the initial abdominal entry.
Proper documentation
Create an accurate record of the laparoscopy, including normal and abnormal findings, by either videotaping the procedure or creating prints or slides. Compose pictures with a clear anatomic frame of reference. Also, be sure to precede close-up images with a panoramic view, so that all anatomic relationships will be clear.
Both the methodical approach to the laparoscopy itself and the visual documentation you’ve created will help you produce a complete and accurate operative report. It is much easier to recall details when a systematic method has been used. Pictures or videos will further serve to refresh the memory.
RECOMMENDED READING
- Hulka JF, Reich H, eds. Textbook of Laparoscopy. 3rd ed. Philadelphia: W.B. Saunders; 1998.
- Suttton C, Diamond M, eds. Endoscopic Surgery for Gynecologists. 2nd ed. Philadelphia: W.B. Saunders; 1998.
- Nezhat CR, Nezhat CH, Nezhat F, Luciano AA, Siegler AM, Metzger DA. Operative Gynecologic Laparoscopy. New York: McGraw-Hill; 1995.
- Council on Resident Education in Obstetrics and Gynecology. Advanced Surgical Techniques for Residency Training Programs in Obstetrics and Gynecology. CREOG Training Guidelines. Washington, DC: CREOG; 1994.
Dr. George serves as a faculty member in preceptorship programs funded by Ethicon Endo Surgery.
