Examining the “Repletion Reflex”: The Association between Serum Potassium and Outcomes in Hospitalized Patients with Heart Failure





BACKGROUND: In patients hospitalized with heart failure (HF) exacerbations, physicians routinely supplement potassium to maintain levels ≥4.0 mEq/L. The evidence basis for this practice is relatively weak. We aimed to evaluate the association between serum potassium levels and outcomes in patients hospitalized with HF.
METHODS: We identified patients admitted with acute HF exacerbations to hospitals that contributed to an electronic health record-derived dataset. In a subset of patients with normal admission serum potassium (3.5-5.0 mEq/L), we averaged serum potassium values during a 72-hour exposure window and categorized as follows: <4.0 mEq/L (low normal), 4.0-4.5 mEq/L (medium normal), and >4.5 mEq/L (high normal). We created multivariable models examining associations between these categories and outcomes.
RESULTS: We included 4,995 patients: 2,080 (41.6%), 2,326 (46.6%), and 589 (11.8%) in the <4.0, 4.0-4.5, and >4.5 mEq/L cohorts, respectively. After adjustment for demographics, comorbidities, and presenting severity, we observed no difference in outcomes between the low and medium normal groups. Compared to patients with levels <4.0 mEq/L, patients with a potassium level of >4.5 mEq/L had a longer length of stay (median of 0.6 days; 95% CI: 0.1 to 1.0) but did not have statistically significant increases in mortality (OR [odds ratio] = 1.51; 95% CI: 0.97 to 2.36) or transfers to the intensive care unit (OR = 1.78; 95% CI: 0.98 to 3.26).
CONCLUSIONS: Inpatients with heart failure who had mean serum potassium levels of <4.0 showed similar outcomes to those with mean serum potassium values of 4.0-4.5. Compared with mean serum potassium level of <4.0, mean serum levels of >4.5 may be associated with increased risk of poor outcomes.
© 2019 Society of Hospital Medicine
Serum Potassium Values
Individuals’ mean serum potassium within the 72-hour exposure window ranged from 2.9 to 5.8 mEq/L (Table 2). In the <4.0, 4-4.5, and >4.5 mEq/L cohorts respectively, patients had a median serum potassium of 3.8 mEq/L (2.9-3.9), 4.2 mEq/L (4.0-4.5), and 4.7 mEq/L (4.5-5.8) during the exposure window. Approximately half of the patients in the <4.0 mEq/L group had a serum potassium <3.5 mEq/L at some point during the exposure window. In contrast, <10% of the other groups had this low value during the exposure window.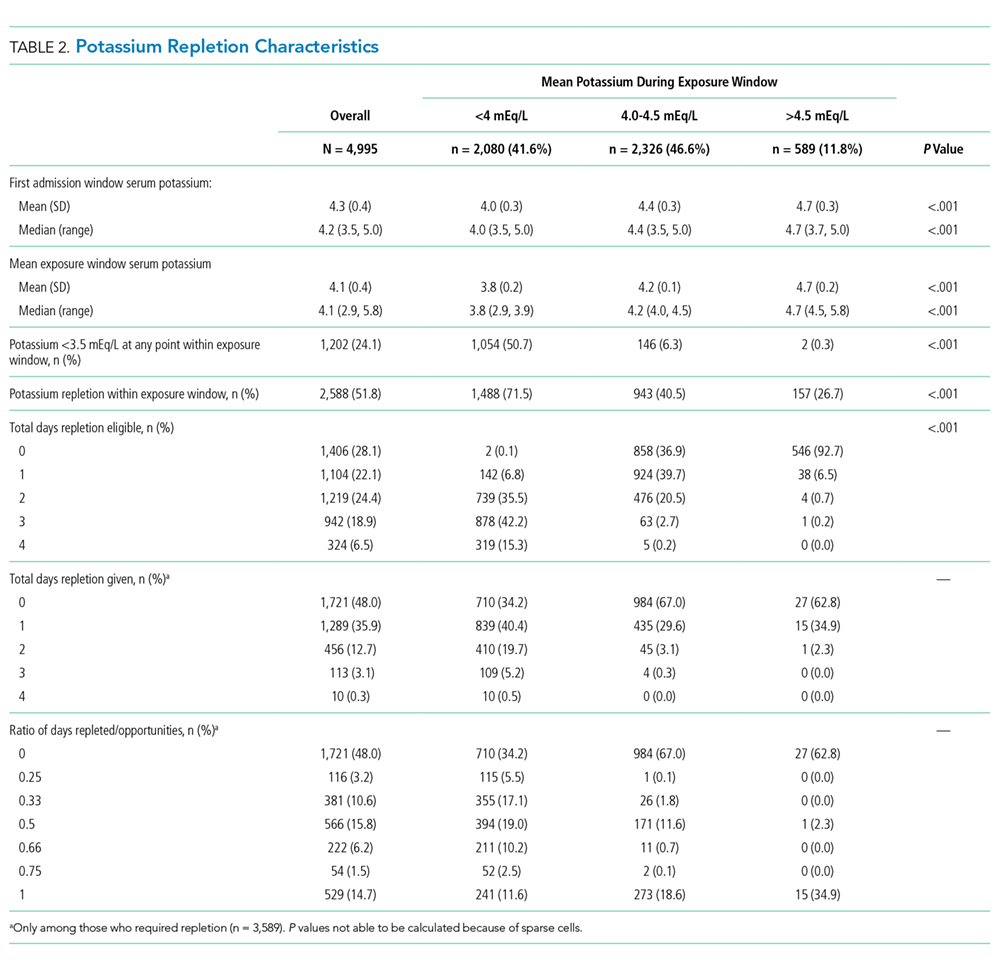
Potassium Repletion
Patients in the <4.0 mEq/L group were much more likely to receive potassium repletion during the exposure window when compared with the 4.0-4.5 mEq/L (71.5% vs 40.5%) and >4.5 mEq/L (71.5% vs 26.7%) groups. On days that they were eligible for repletion (defined as a daily potassium value <4.0 mEq/L), patients with mean serum potassium >4.0 mEq/L were less likely to receive potassium repletion compared with those with values <4.0 mEq/L. There were 592 (28.5%), 1,383 (59.5%), and 432 (73.3%) patients in the <4.0, 4-4.5, and >4,5 mEq/L groups, respectively, who did not receive potassium repletion therapy during the exposure window.
Relationship of Serum Potassium Levels and Outcomes
Overall, 3.7% (n = 187) of patients died during the hospitalization, 2.4% (n = 98) were admitted to the ICU after the exposure window, and the median LOS was 5.6 days. We did not observe a significant association between mean serum potassium of <4.0 or 4.0-4.5 mEq/L and increased risk of mortality, ICU transfer, or LOS (Table 3). Our unadjusted analysis showed that patients with values >4.5 mEq/L had worse outcomes, including more deaths (5.3%; OR = 1.55; 95% CI: 1.01 to 2.39) and ICU admission (3.8%; OR = 2.10; 95% CI: 1.16 to 3.80) compared with those with values <4.0 mEq/L (Table 3). We also found that, compared with the <4.0 mEq/L group, the >4.5 mEq/L group showed just over a half-day longer LOS (0.6 days; 95% CI: 0.0 to 1.0; Table 3). However, we found that mortality and ICU admission results were attenuated after adjustment for age, race, comorbidity score, and LAPS-2 and were no longer statistically significant, whereas the association with LOS was consistent after adjustment. When using a binary exposure (<4.0 versus ≥4.0 mEq/L), we observed no association between mean potassium value and increased risk of mortality, ICU transfer, or LOS both before and after adjustment for age, race, LAPS-2, and comorbidity score (data not shown).
Sensitivity Analyses
In the sensitivity analysis restricted to those who did not receive potassium repletion during the exposure window, we continued to observe no association between the <4.0 and 4.0-4.5 mEq/L groups and outcomes (Table 3). In adjusted models for the >4.5 versus <4.0 mEq/L groups, risk estimates for mortality were similar to the full sample, but statistical significance was lost (OR = 1.56; 95% CI: 0.81 to 3.01). Adjusted risk estimates for ICU transfer were attenuated and not statistically significant (OR = 1.40; 95% CI: 0.60 to 3.26). However, LOS estimates were very similar to that observed in the full dataset (0.6 days; 95% CI: 0.1 to 1.2).