Examining the “Repletion Reflex”: The Association between Serum Potassium and Outcomes in Hospitalized Patients with Heart Failure





BACKGROUND: In patients hospitalized with heart failure (HF) exacerbations, physicians routinely supplement potassium to maintain levels ≥4.0 mEq/L. The evidence basis for this practice is relatively weak. We aimed to evaluate the association between serum potassium levels and outcomes in patients hospitalized with HF.
METHODS: We identified patients admitted with acute HF exacerbations to hospitals that contributed to an electronic health record-derived dataset. In a subset of patients with normal admission serum potassium (3.5-5.0 mEq/L), we averaged serum potassium values during a 72-hour exposure window and categorized as follows: <4.0 mEq/L (low normal), 4.0-4.5 mEq/L (medium normal), and >4.5 mEq/L (high normal). We created multivariable models examining associations between these categories and outcomes.
RESULTS: We included 4,995 patients: 2,080 (41.6%), 2,326 (46.6%), and 589 (11.8%) in the <4.0, 4.0-4.5, and >4.5 mEq/L cohorts, respectively. After adjustment for demographics, comorbidities, and presenting severity, we observed no difference in outcomes between the low and medium normal groups. Compared to patients with levels <4.0 mEq/L, patients with a potassium level of >4.5 mEq/L had a longer length of stay (median of 0.6 days; 95% CI: 0.1 to 1.0) but did not have statistically significant increases in mortality (OR [odds ratio] = 1.51; 95% CI: 0.97 to 2.36) or transfers to the intensive care unit (OR = 1.78; 95% CI: 0.98 to 3.26).
CONCLUSIONS: Inpatients with heart failure who had mean serum potassium levels of <4.0 showed similar outcomes to those with mean serum potassium values of 4.0-4.5. Compared with mean serum potassium level of <4.0, mean serum levels of >4.5 may be associated with increased risk of poor outcomes.
© 2019 Society of Hospital Medicine
Potassium Repletion
Analysis
We evaluated the differences in patient characteristics across serum potassium categories. Categorical variables are presented as frequencies and percentages, whereas continuous variables are presented as means and standard deviations. For binary outcomes, we used generalized estimating equations (with a binomial family and logit link and clustering by hospital) to estimate incidence and calculate unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs). For LOS, we estimated the median and 95% CIs using quantile regression with clustered standard errors.24 We calculated all models using both a binary exposure (<4.0 versus ≥4.0 mEq/L) and a three-level categorization (<4.0, 4.0-4.5, and >4.5 mEq/L) to explore the effects at the highest potassium level. We adjusted all models for age, race, LAPS-2 score, and combined comorbidity score. We conducted two sensitivity analyses. First, we restricted our sample to those who never received potassium during the exposure window, as these patients may be different than patients who required potassium repletion. Second, we stratified our findings by the presence or absence of acute or chronic renal insufficiency (defined as an admission creatinine >1 or the presence of a diagnostic code for renal insufficiency, as defined by Elixhauser et al.).19,21 Statistical significance was set at an alpha of 0.05. Analysis was completed using Stata v15.1, StataCorp LP, College Station, Texas.
RESULTS
Cohort Description
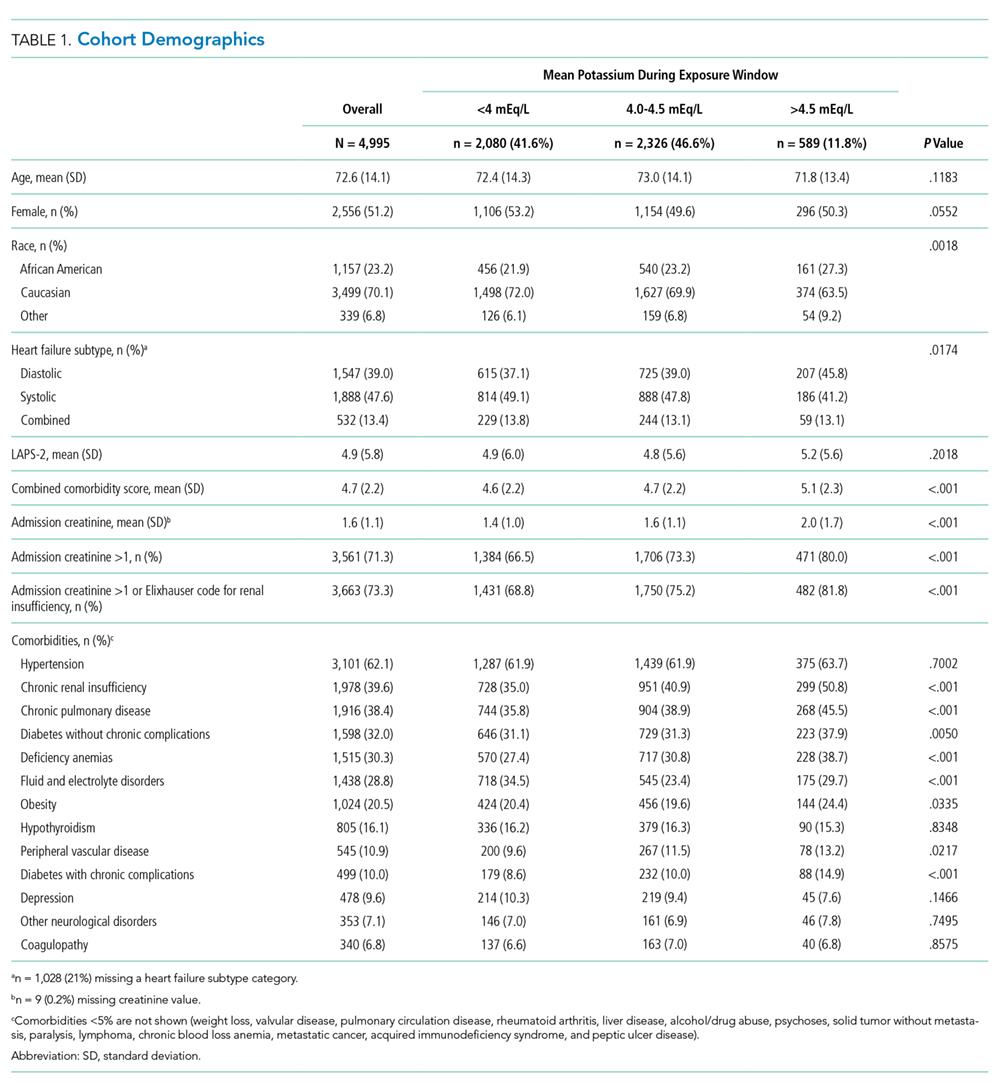
We identified patients from 56 geographically diverse US hospitals, although most were located in either the northeast (n = 21; 38%) or south (n = 18; 32%). A total of 59% of the hospitals were teaching hospitals, and nearly 95% were in an urban setting. We identified 13,163 patients with HF, of which 4,995 (38.0%) met the inclusion criteria. We excluded 3,744 (28.4%) patients with LOS < 72 hours, 2,210 (16.8%) with admission potassium values outside of the defined range, and 896 (6.8%) with fewer than three potassium values during the exposure window. Of the patients who met the inclusion criteria, 2,080 (41.6%), 2,326 (46.6%), and 589 (11.8%) were categorized in the <4.0, 4.0-4.5, and >4.5 mEq/L groups, respectively (Table 1). The groups were clinically similar in terms of age, sex, illness severity (LAPS-2), and comorbidity score. Compared with other racial groups, black patients had higher potassium values. While the <4.0 and 4.0-4.5 mEq/L groups were relatively similar, the group with mean potassium >4.5 mEq/L had higher admission creatinine and a greater prevalence of chronic kidney disease, deficiency anemias, and chronic obstructive pulmonary disease (Table 1).