Association between Inpatient Delirium and Hospital Readmission in Patients ≥ 65 Years of Age: A Retrospective Cohort Study





BACKGROUND: Delirium affects more than seven million hospitalized adults in the United States annually. However, its impact on postdischarge healthcare utilization remains unclear.
OBJECTIVE: To determine the association between delirium and 30-day hospital readmission.
DESIGN: A retrospective cohort study.
SETTING: A general community medical and surgical hospital.
PATIENTS: All adults who were at least 65 years old, without a history of delirium or alcohol-related delirium, and were hospitalized from September 2010 to March 2015.
MEASUREMENTS: The patients deemed at risk for or displaying symptoms of delirium were screened by nurses using the Confusion Assessment Method with a follow-up by a staff psychiatrist for a subset of screen-positive patients. Patients with delirium confirmed by a staff psychiatrist were compared with those without delirium. The primary outcome was the 30-day readmission rate. The secondary outcomes included emergency department (ED) visits 30 days postdischarge, mortality during hospitalization and 30 days postdischarge, and discharge location.
RESULTS: The cohort included 718 delirious patients and 7,927 nondelirious patients. Using an unweighted multivariable logistic regression, delirium was determined to be significantly associated with the increased odds of readmission within 30 days of discharge (odds ratio (OR): 2.60; 95% CI, 1.96-3.44; P < .0001). Delirium was also significantly (P < .0001) associated with ED visits within 30 days postdischarge (OR: 2.18; 95% CI: 1.77-2.69) and discharge to a facility (OR: 2.52; 95% CI: 2.09-3.01).
CONCLUSIONS: Delirium is a significant predictor of hospital readmission, ED visits, and discharge to a location other than home. Delirious patients should be targeted to reduce postdischarge healthcare utilization.
© 2019 Society of Hospital Medicine
Patient Characteristics
Patient demographics and clinical data were obtained from the electronic medical records. We used several scores to characterize illness severity, including the Charlson comorbidity index,27 Laboratory-Based Acute Physiology, version 2 (LAPS2) score28—an externally validated score for acute severity of illness—and disease categories as defined by the Healthcare Cost and Utilization Project (HCUP).29
Outcomes
The primary outcome was the rate of readmission to the hospital within 30 days of discharge from the hospitalization in which delirium was first diagnosed. Readmissions and ED visits to any Kaiser Permanente hospital and to hospitals outside of the Kaiser Permanente network with Kaiser Permanente insurance were captured. To avoid incorrectly coding patients transferred from the index hospital to another hospital as readmissions, we excluded readmissions that occurred on the day of discharge or the following calendar day. This action was expected to lower the absolute number of readmissions but restrict the analysis to true readmissions. The models of postdischarge outcomes are based on the subset of patients discharged alive. The secondary outcome measures included discharge from the index hospitalization to a skilled nursing facility or hospice rather than to home and emergency room visits within 30 days of discharge. We also quantified rates of mortality during hospitalization and at 30 days postdischarge.
Statistical Analysis
Comparisons between patients with delirium and those without were performed using Pearson’s X2 test for categorical variables and student t-test for continuous variables. The estimated odds of our outcome measures for delirious and nondelirious subjects were calculated from multivariable logistic regression models, which controlled for predictors of delirium and additional information obtained during the hospitalization. For inpatient outcomes (in-hospital mortality and discharge to skilled nursing facility or hospice), we adjusted only for admission characteristics: age, race/ethnicity, admission to ICU, Charlson comorbidity index, HCUP category, and admission category. To limit the number of variables in our model, we consolidated the initial 30 HCUP categories (Appendix Table 1) by illness type into 13 categories (Appendix Table 2). For postdischarge outcomes, we adjusted for all the variables, including disposition (Table 2). The average estimated odds were calculated based on the observed marginal distribution of the control variables. The P value indicates how likely the odds on each outcome for delirious subjects differed significantly from those for other subjects. All statistical analyses were performed using SAS 9.3 (SAS Institute Inc., Cary, North Carolina).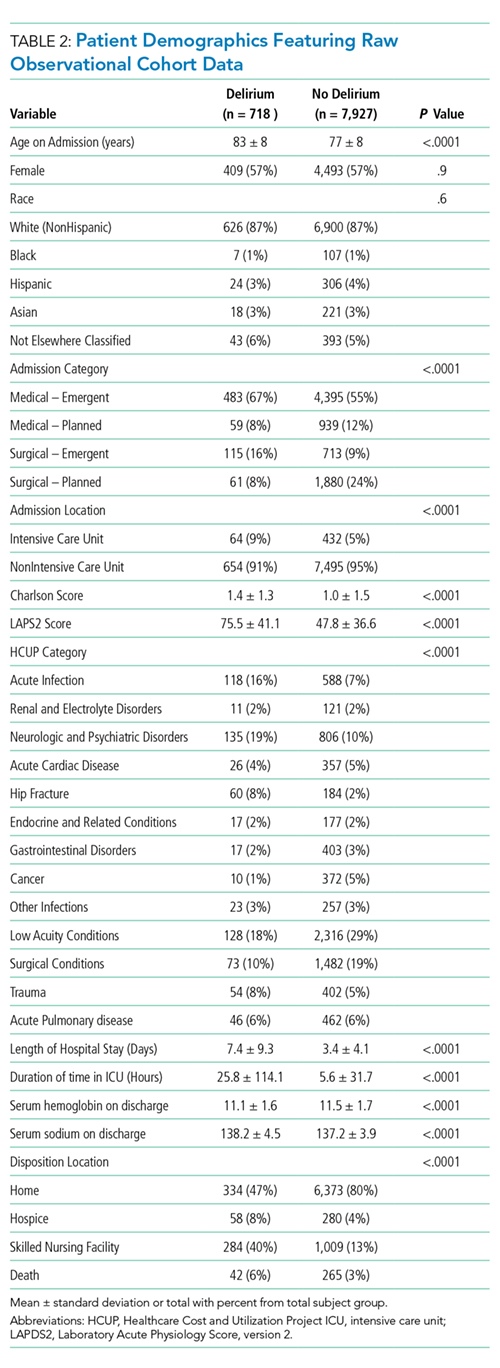
RESULTS
Demographics and Clinical Characteristics
A total of 718 patients with delirium and 7,927 patients without delirium were included in this study. The related demographic information is outlined in Table 2. On average, the patients with delirium were older (83 ± 8 years versus 77 ± 8 years, P < .0001) but no difference in gender distribution was observed between groups. A similar racial breakdown was noted between groups, with white patients accounting for 87% of both patients with delirium and those without. The majority of admissions were unplanned medical admissions. The delirium cohort included more emergent surgical admissions compared with patients who did not develop delirium. Patients who developed delirium exhibited higher levels of illness severity on admission, as measured by the Charlson and LAPS2 scores, and were more often admitted to the ICU. Significant differences were also observed between admission illness categories between patients with delirium and those without.
