Readmissions after Pediatric Hospitalization for Suicide Ideation and Suicide Attempt





OBJECTIVE: To inform resource allocation toward a continuum of care for youth at risk of suicide, we examined unplanned 30-day readmissions after pediatric hospitalization for either suicide ideation (SI) or suicide attempt (SA).
METHODS: We conducted a retrospective cohort study of a nationally representative sample of 133,516 hospitalizations for SI or SA among 6- to 17-year-olds to determine prevalence, risk factors, and characteristics of 30-day readmissions using the 2013 and 2014 Nationwide Readmissions Dataset (NRD). Risk factors for readmission were modeled using logistic regression.
RESULTS: We identified 95,354 hospitalizations for SI and 38,162 hospitalizations for SA. Readmission rates within 30 days were 8.5% for SI and SA hospitalizations. Among 30-day readmissions, more than one-third (34.1%) occurred within 7 days. Among patients with any 30-day readmission, 11% had more than one readmission within 30 days. The strongest risk factors for readmission were SI or SA hospitalization in the 30 days preceding the index SI/SA hospitalization (adjusted odds ratio [AOR]: 3.14, 95% CI: 2.73-3.61) and hospitalization for other indications in the previous 30 days (AOR: 3.18, 95% CI: 2.67-3.78). Among readmissions, 94.5% were for a psychiatric condition and 63.4% had a diagnosis of SI or SA.
CONCLUSIONS: Quality improvement interventions to reduce unplanned 30-day readmissions among children hospitalized for SI or SA should focus on children with a recent prior hospitalization and should be targeted to the first week following hospital discharge.
© 2018 Society of Hospital Medicine
Statistical Analysis
We compared descriptive, summary statistics for characteristics of index hospitalizations with and without a 30-day readmission using Rao-Scott chi-square tests. In multivariable analyses, we derived logistic regression models to measure the associations of patient, hospital, and temporal factors with 30-day hospital readmissions. Analyses were conducted in SAS PROC SURVEYLOGISTIC and were weighted to achieve national estimates, clustered by sample stratum and hospital to account for the complex survey design,27 clustered by patients to account for multiple index visits per patient, and adjusted for clinical, demographic, and hospital characteristics. SAS version 9.4 (SAS Institute, Cary, North Carolina) was used for all analyses. All tests were two-sided, and a P value <.05 was considered as statistically significant.
RESULTS
Sample Characteristics
In the weighted analyses, we identified 133,516 hospitalizations in acute-care hospitals for SI or SA, and 8.5% (n = 11,375) of hospitalizations had at least one unplanned 30-day readmission to an acute-care hospital. Unweighted, the sample included 37,683 patients and 42,198 hospitalizations. Among all patients represented in the sample, 90.5% had only a single SI or SA hospitalization, 7.7% had two hospitalizations, and 1.8% had >2 hospitalizations in one year.
Table 1 summarizes the sample characteristics and displays the demographic, clinical, and hospital characteristics of index hospitalizations by the 30-day readmission status. Patients represented in the index hospitalizations were 64.9% female, 3.6% were aged 6-9 years, 40.1% were aged 10-14 years, and 56.3% were aged 15-17 years. Nearly half of the patients (49.1%) used public insurance. Nearly half (44.9%) lived in metropolitan areas with >1 million residents, 36.1% lived in metropolitan areas with 50,000 to 1 million residents, and 14.7% lived in rural areas.
Median length of stay for the index hospitalization was 5 days (interquartile range [IQR] 3-7). Nearly one-third (32.3%) of patients had a noncomplex chronic medical condition, 7.8% had a complex chronic medical condition, and 98.1% had a psychiatric condition. The most common psychiatric conditions were depressive disorders (60.0%) and anxiety disorders (42.2%). More than half (55.0%) of the patients had >2 psychiatric conditions. Most hospitalizations in the sample had SI only (71.4%). Among patients with SA, 81.0% had a lower lethality mechanism of injury and 19.0% had a higher lethality mechanism.
Patients experiencing a readmission were more likely to be 10-14 years old and use public insurance than patients without a readmission (P < .001 for both). For clinical characteristics, patients with a readmission were more likely to have longer index hospital stays (6 vs. 5 days), >2 psychiatric conditions (SI vs. SA), a prior admission in the 30 days preceding the index hospitalization, and admission via the ED (vs. direct admission) (P < .001 for all).
Association of Patient and Hospital Characteristics with Readmissions
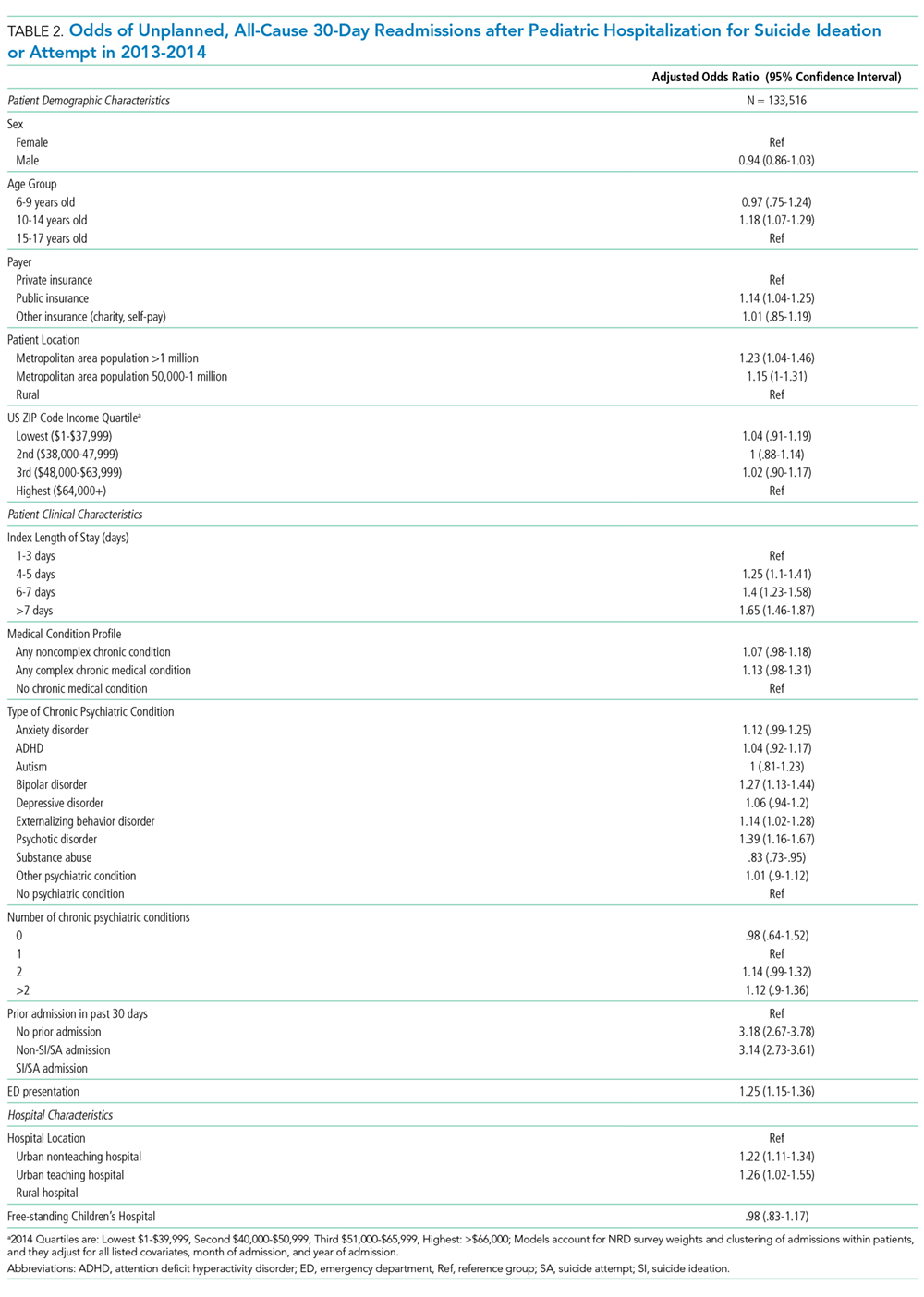
Table 2 displays the patient and hospital characteristics associated with readmissions. Among demographic characteristics, 10- to 14-year-old patients had higher odds of readmission (odds ratio [OR]: 1.18, 95% confidence interval [CI]: 1.07-1.29) than 15- to 17-year-old patients. Having public insurance was associated with higher odds of readmission (OR: 1.14, 95% CI: 1.04-1.25). We found no differences in readmission rates based on sex, urban or rural location, or patient’s ZIP code income quartile.