Readmissions after Pediatric Hospitalization for Suicide Ideation and Suicide Attempt





OBJECTIVE: To inform resource allocation toward a continuum of care for youth at risk of suicide, we examined unplanned 30-day readmissions after pediatric hospitalization for either suicide ideation (SI) or suicide attempt (SA).
METHODS: We conducted a retrospective cohort study of a nationally representative sample of 133,516 hospitalizations for SI or SA among 6- to 17-year-olds to determine prevalence, risk factors, and characteristics of 30-day readmissions using the 2013 and 2014 Nationwide Readmissions Dataset (NRD). Risk factors for readmission were modeled using logistic regression.
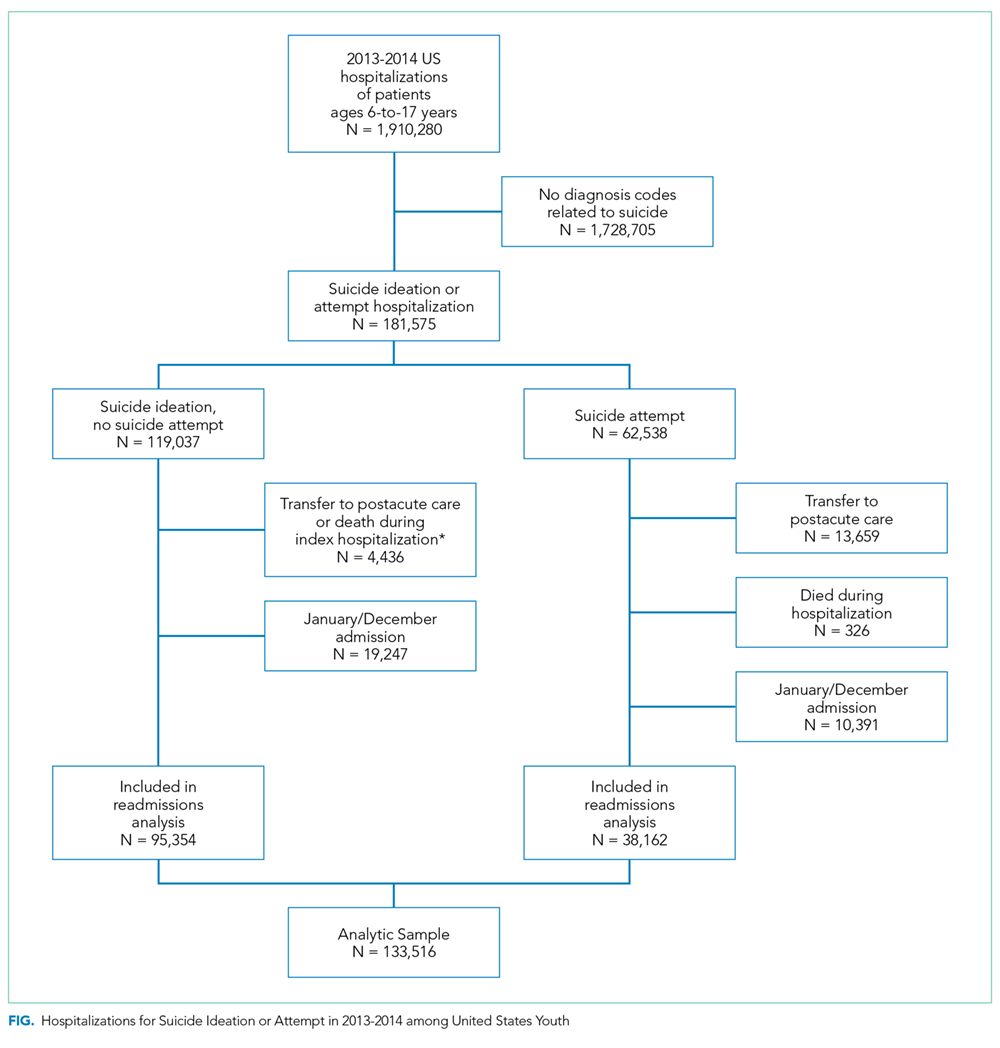
RESULTS: We identified 95,354 hospitalizations for SI and 38,162 hospitalizations for SA. Readmission rates within 30 days were 8.5% for SI and SA hospitalizations. Among 30-day readmissions, more than one-third (34.1%) occurred within 7 days. Among patients with any 30-day readmission, 11% had more than one readmission within 30 days. The strongest risk factors for readmission were SI or SA hospitalization in the 30 days preceding the index SI/SA hospitalization (adjusted odds ratio [AOR]: 3.14, 95% CI: 2.73-3.61) and hospitalization for other indications in the previous 30 days (AOR: 3.18, 95% CI: 2.67-3.78). Among readmissions, 94.5% were for a psychiatric condition and 63.4% had a diagnosis of SI or SA.
CONCLUSIONS: Quality improvement interventions to reduce unplanned 30-day readmissions among children hospitalized for SI or SA should focus on children with a recent prior hospitalization and should be targeted to the first week following hospital discharge.
© 2018 Society of Hospital Medicine
The National Committee on Quality Assurance recommends measurement of quality metrics for 30-day mental health follow-up after psychiatric hospitalizations, 30-day readmissions after adult (but not pediatric) psychiatric hospitalizations, and 30-day readmissions in pediatric medical and surgical hospitalizations. Readmission measures are not consistently used to evaluate pediatric psychiatric hospitalizations, and psychiatric quality measures are not used to evaluate medical or surgical hospitalizations for SA. Recent research has investigated transfers to postacute care,8 readmission prevalence, variation in hospital readmission performance, and risk factors for readmissions after pediatric psychiatric hospitalizations.9–11 However, no national study has investigated 30-day readmissions in youth hospitalized specifically for SI or SA.
To inform hospital quality measurement and improve hospital and postdischarge care for youth at risk of suicide, more information is needed about the characteristics of and the risk factors for readmissions after index SI/SA hospitalization. To address this knowledge gap, among SI/SA hospitalizations in 6- to 17-year-olds, we examined (1) unplanned 30-day readmissions and characteristics of hospitalizations by 30-day readmission status; (2) patient, hospital, and regional characteristics associated with 30-day readmissions; and (3) characteristics of 30-day readmissions.
METHODS
Study Design and Data Source
We conducted a national, retrospective cohort study of hospitalizations for patients aged 6-17 years using the Agency for Healthcare Research and Quality (AHRQ) 2013 and 2014 Nationwide Readmissions Database (NRD). The combined 2013-2014 NRD includes administrative data from a nationally representative sample of 29 million hospitalizations in 22 states, accounting for 49.3% of all US hospitalizations, and is weighted for national projections. The NRD includes hospital information, patient demographic information, and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis, procedure, and external cause of injury codes (E-codes). The database includes one primary diagnosis, up to 24 additional diagnoses, and up to 4 E-codes for each hospitalization. The NRD includes information about hospitalizations in acute-care general hospitals (including their psychiatric units) but not from specialty psychiatric hospitals. The database also includes de-identified, verified patient linkage numbers so that patients can be tracked across multiple hospitalizations at the same institution or different institutions within the same state. This study was considered to be exempt from review by the Children’s Hospital of Philadelphia Institutional Review Board.
Sample
We identified a sample of 181,575 hospitalizations for SI (n = 119,037) or SA (n = 62,538) among 6- to 17-year-olds between January 1, 2013, and December 31, 2014 (Figure). We included children as young as 6 years because validated methods exist to identify SI and SA in this age group,12 and because suicide deaths have recently increased among younger children.3 We excluded patients aged 18 years and older from this study since delivery of mental health services differs for adults.13 To create the sample, we first identified all hospitalizations of patients aged 6-17 years. We then used a validated algorithm relying on ICD-9-CM diagnosis codes for poisonings and E-codes for self-injury (E950-959) to identify hospitalizations related to SA.12 Because E-code completeness varies among states,14 we also used the combination of having both a diagnosis code for injury (800-999) and an ICD-9-CM code for SI (V62.84) as a proxy for SA. Among hospitalizations without SA, we identified hospitalizations with SI using the ICD-9-CM code for SI (V62.84) in any position.