Perspectives of Clinicians at Skilled Nursing Facilities on 30-Day Hospital Readmissions: A Qualitative Study





BACKGROUND: Unplanned 30-day hospital readmissions are an important measure of hospital quality and a focus of national regulations. Skilled nursing facilities (SNFs) play an important role in the readmission process, but few studies have examined the factors that contribute to readmissions from SNFs, leaving hospitalists and other hospital-based clinicians with limited evidence on how to reduce SNF readmissions.
OBJECTIVE: To understand the perspectives of clinicians working at SNFs regarding factors contributing to readmissions.
DESIGN AND PARTICIPANTS: We prospectively identified consecutive readmissions from SNFs to a single tertiary-care hospital. Index admissions and readmissions were to the hospital’s inpatient general medicine service. SNF clinicians who cared for the readmitted patients were identified and interviewed about root causes of the readmissions using a structured interview tool. Transcripts of the interviews were inductively analyzed using grounded theory methodology.
RESULTS: We interviewed 28 clinicians at 15 SNFs. The interviews covered 24 patient readmissions. SNF clinicians described a range of procedural, technological, and cultural contributors to unplanned readmissions. Commonly cited causes of readmission included a lack of coordination between emergency departments and SNFs, poorly defined goals of care at the time of hospital discharge, acute illness at the time of hospital discharge, limited information sharing between a SNF and hospital, and SNF process and cultural factors.
CONCLUSION: SNF clinicians identified a broad range of factors that contribute to readmissions. Addressing these factors may mitigate patients’ risk of readmission from SNFs to acute care hospitals. Journal of Hospital Medicine 2017;12:632-638. © 2017 Society of Hospital Medicine
© 2017 Society of Hospital Medicine
Skilled nursing facilities (SNFs) play a crucial role in the hospital readmission process.Approximately 1 in 4 Medicare beneficiaries discharged from an acute care hospital is admitted to a SNF instead of returning directly home. Of these patients, 1 in 4 will be readmitted within 30 days,1 a rate significantly higher than the readmission rate of the inpatient population as a whole.2 The 2014 Protecting Access to Medicare Act created a value-based purchasing program that will use quality measures to steer funds to, or away from, individual SNFs. When the program takes effect in 2018, the Centers for Medicare & Medicaid Services will use SNFs’ 30-day all-cause readmission rate to determine which SNFs receive payments and which receive penalties.3 The Affordable Care Act, passed in 2010, has also established penalties for hospitals with higher than expected readmission rates for Medicare patients.4
Despite this intensifying regulatory focus, relatively little is known about the factors that drive readmissions from SNFs. A prospective review of data from SNFs in 4 states has shown that SNFs staffed by nurse practitioners or physician assistants and those equipped to provide intravenous therapy were less likely to transfer patients to the hospital for ambulatory care-sensitive diagnoses.5 Qualitative studies have provided useful insight into the causes of SNF-to-hospital transfers but have not focused on 30-day readmissions.6,7 A single survey-based study has examined the causes of SNF-to-hospital readmissions.8 However, survey-based methodologies have limited ability to capture the complex perspectives of SNF clinicians, who play a critical role in determining which SNF patients require evaluation or treatment in an acute care setting.
To address this gap in knowledge about factors contributing to SNF readmissions, we conducted a qualitative study examining SNF clinicians’ perspectives on patients readmitted to the hospital within 30 days of discharge. We used a structured interview tool to explore the root causes of readmission with frontline SNF staff, with the goal of using this knowledge to inform future hospital quality improvement (QI) efforts.
METHODS
Case Identification
Hospital data-tracking software (Allscripts) was used to identify patients who experienced a 30-day, unplanned readmission from SNFs to an academic medical center. We restricted our search to patients whose index admission and readmission were to the medical center’s inpatient general medicine service. A study team member (BWC) monitored the dataset on a weekly basis and contacted SNF clinicians by e-mail and telephone to arrange interviews at times of mutual convenience. To mitigate against recall bias, interviews were conducted within 30 days of the readmission in question. A total of 32 cases were identified. No SNF clinicians refused a request for interview. For 8 of these cases, it was not possible to find a time of mutual convenience within the specified 30-day window. The remaining 24 cases involved patients from 15 SNFs across Connecticut. Interviews were conducted from August 2015 to November 2015.
The project was reviewed by our institution’s Human Investigation Committee and was exempted from Institutional Review Board review.
Study Participants
Interviews were conducted on-site at SNFs with groups of 1 to 4 SNF clinicians and administrators. SNF participants were informed of interviewer credentials and the study’s QI goals prior to participation. Participation was voluntary and did not affect the clinician’s relationship with the hospital or the SNF. Participants were not paid.
DATA COLLECTION
Interventions to Reduce Acute Care Transfers (INTERACT) is a QI program that includes training for clinicians, communication tools, and advance care planning tools.9 INTERACT is currently used in 138 Connecticut SNFs as part of a statewide QI effort funded by the Connecticut State Department of Public Health. In prospective QI studies,10,11 implementation of INTERACT has been associated with decreased transfers from SNFs to acute care hospitals. The INTERACT Quality Improvement Tool, one part of the INTERACT bundle of interventions, is a 26-item questionnaire used to identify root causes of transfers from SNFs to acute care hospitals. It includes both checklists and open-ended questions about patient factors, SNF procedures, and SNF clinical decision-making.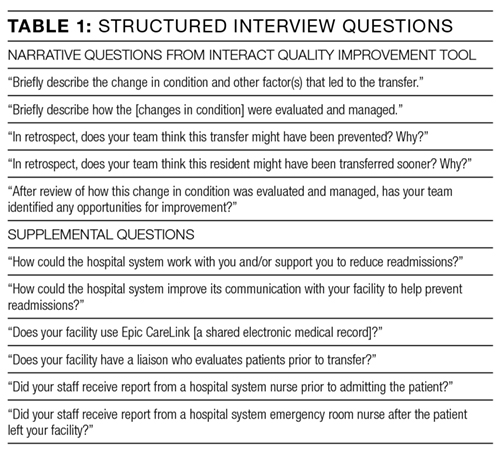
We used the INTERACT QI Tool12 to conduct structured interviews with nurses and administrators at SNFs. Interviewers used a hard copy of the tool to maintain field notes, and all parts of the questionnaire were completed in each interview. Although the questionnaire elicits baseline demographic and medical information, such as the patient’s age and vital signs prior to readmission, the majority of each interview was dedicated to discussion of the open-ended questions in Table 1. Upon completion of the INTERACT QI Tool, the interviewer asked 2 open-ended questions about reducing readmissions and 4 closed-ended questions regarding SNF admission procedures. (Table 1) The supplemental questions were added after preliminary interviews with SNF clinicians revealed concerns about the SNF referral process and about communication between the hospital, emergency department (ED) and SNFs—issues not included in the INTERACT questionnaire. Interviewers used phatic communication, probing questions, and follow-up questions to elicit detailed information from participants, and participant responses were not limited to topics in the questionnaire and the list of supplemental questions.
Interviews were conducted by a hospital clinical integration coordinator, social worker, and a physician (KB, MCB, BWC). All interviewers received formal training in qualitative research methods prior to the study.
All interviews were audio recorded, with permission from the participants, and were professionally transcribed. Field notes were maintained to ensure accuracy of INTERACT QI Tool data. Participant interviews covered no more than two cases per session and lasted from 18 to 71 minutes (mean duration, 38 minutes).