Physician Responsiveness to Positive Blood Culture Results at the Minneapolis Veterans Affairs Hospital—Is Anyone Paying Attention?





Background: Patients presenting with suspected infections are typically placed on empiric broad-spectrum antibiotics. With mounting evidence supporting the efficacy of using the narrowest spectrum of antimicrobial therapy to cover the suspected pathogen, current guidelines recommend decreasing the breadth of coverage in response to culture results both in relation to microbe identification and antibiotic sensitivity.
Methods: A retrospective chart review of electronic health records at the Minneapolis Veterans Affairs Medical Center (VAMC) in Minnesota was performed for 208 positive blood cultures with antibiotic spectrum analysis from July 1, 2015 to June 30, 2016. The time of reporting for pathogen identification and subsequent pathogen susceptibilities were compared to the time at which any alterations to antibiotic coverage were made. The breadth of antibiotic coverage was recorded using a nonlinear spectrum score. The use of this score allowed for the reliable classification of antibiotic adjustments as either deescalation, escalation, or no change.
Results: The percentage of cases deescalated was higher in response to physician (house staff or attending physician) notification of pathogen susceptibility information when compared with a response to pathogen identification alone (33.2% vs 22.6%). Empiric antibiotics were not altered within 24 hours in response to pathogen identification in 70.7% of cases and were not altered within 24 hours in response to pathogen sensitivity determination in 58.6% of cases. However, when considering the time frame from when empiric antibiotics were started to 24 hours after notification of susceptibility information, 49.5% of cases were deescalated and 41.5% of cases had no net change in the antibiotic spectrum score. The magnitude of deescalations were notably larger than escalations. The mean (SD) time to deescalation of antibiotic coverage was shorter ( P =.049) in response to pathogen identification at 8 (7.4) hours compared with sensitivity information at 10.4 (7) hours, but may not be clinically relevant.
Conclusion: Health care providers at the Minneapolis VAMC appear to be using positive blood culture results in a timely fashion consistent with best practices. Because empirically initiated antibiotics typically are broad in spectrum, the magnitude of deescalations were notably larger than escalations. Adherence to these standards may be a reflection of the infectious disease staff oversight of antibiotic administration. Furthermore, the systems outlined in this quality improvement study may be replicated at other VAMCs across the country by either in-house infectious disease staff or through remote monitoring of the electronic health record by other infectious disease experts at a more centralized VAMC. Widespread adoption throughout the Veterans Health Administration may result in improved antibiotic resistance profiles and better clinical outcomes for our nation’s veterans
Another finding within this investigation was the statistically significantly shorter response mean (SD) time when deescalating in response to pathogen identification (8 [7.3] h) than to sensitivity profile (10.4 [7] h). Overall when deescalating, the time of each individual response to antibiotic changes was highly irregular. There was no noticeable time point where a change was more likely to occur within the 24 hours after notification of a culture result. This erratic distribution further exemplifies the complexity of deescalation as it underscores the unique nature of each case. The timing of the dosage of previous antibiotics, the health status of the patient, and the individual physician attitudes about the progression and severity of the infection all likely played into this distribution.
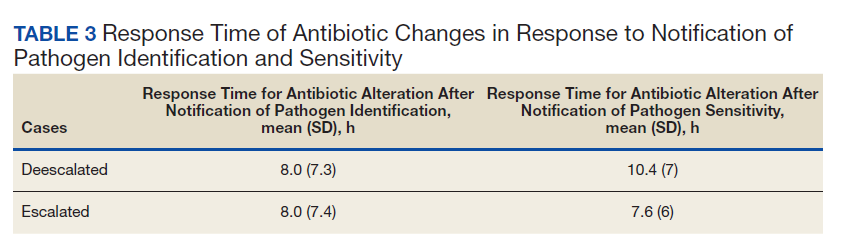
Due to the lack of a regular or even skewed distribution, a Wilcoxon nonparametric rank sum test was performed (P = .049). Although this result was statistically significant, the 2.5-hour time difference is likely clinically irrelevant as both times represent fairly prompt physician responsiveness.50 Nonetheless, it suggests that it was more important to rapidly escalate the breadth of coverage for a patient with a positive blood culture than to deescalate as identified pathogens may have been left untreated with the prescribed antibiotic.
Future Study
Similar studies designed using the spectrum score methodology would allow for more meaningful interinstitutional comparison of antibiotic administration through the use of a unified definition of deescalation and escalation. Comparison of deescalation and escalation rates between hospital systems with similar patient populations with and without prompt infectious disease review and phone notification of blood culture results could further verify the value of such a protocol. It could also help determine which empiric antibiotics may be most effective in individual patient morbidity and mortality outcomes, length of stay, costs, and the development of antibiotic resistance. Chou and colleagues found that only 49 of 130 responding VA facilities had antimicrobial stewardship teams in place with even fewer (29) having a formal policy to establish an antimicrobial stewardship program.11 This significant variation in the practices of VA facilities across the nation underscores the benefit to be gained from implementation of value-added protocols such as daily infectious disease case monitoring and microbiology laboratory phone notification of positive blood culture results as it occurs at MVAMC.
They also noted that systems of patient-level antibiotic review, and the presence of at least one full-time infectious disease physician were both associated with a statistically significant decrease in the use of antimicrobials, corroborating the results of this analysis.11 Adapting the current system of infectious disease specialist review of positive blood culture results to use remote monitoring through the EHR could help to defer some of the cost of needing an in-house specialist while retaining the benefit of the oversite.
Another option for study would be a before and after design to determine whether the program of infectious disease specialist review led to increased use of deescalation strategies similar to studies investigating the efficacy of antimicrobial subcommittee implementation.13,20,23,24,26
Conclusions
This analysis of empiric antibiotic use at the MVAMC indicates promising rates of deescalation. The results indicate that the medical service may be right and that positive blood culture results appear to affect clinical decision making in an appropriate and timely fashion. The VA is the largest health care organization in the US. Thus, identifying and propagating effective stewardship practices on a widespread basis can have a significant effect on the public health of the nation.
These data suggest that the program implemented at the MVAMC of phone notification to the primary care team along with daily infectious disease staff monitoring of blood culture information should be widely adopted at sister institutions using either in-house or remote specialist review.