Keloids: Which treatment is best for your patient?






Corticosteroid injections have proven effective for many patients, but other options may be more appropriate depending on the keloid’s location.
In normal tissue, wound healing stops after the wound has been fully epithelialized by keratinocytes, after which the scar tissue contracts to minimal size. However, keloid growth can continue for years.1
Numerous studies have inspired various hypotheses for keloid formation. Studies demonstrating that keloids contain an increased level of immunoglobulins suggest that they may be produced by an abnormal immune reaction. Microscopic examinations of keloids have shown that overabundant endothelial cells occlude microvessels, suggesting that keloids may occur in the context of wound hypoxia. In vitro studies showing that fibroblasts proliferate when cultured with keloidal keratinocytes suggest that keloids may be a result of abnormal epithelial–mesenchymal interactions.6,7 A hypothesis based on the body sites where keloids are observed is that mechanical stretch and tension across a wound may overstimulate collagen production, possibly as a result of mechanoreceptor damage or disorders.8
Treatment: Weighing the options
Due to the complex mechanisms of pathogenesis, many modalities are available for managing keloids, yet no definitive treatment protocols exist. Intradermal, extradermal, or systemic therapies may be used singly, although combination regimens are the most effective in treating keloids and preventing recurrences.5 The TABLE1,3,5,9-14 provides an overview of monotherapeutic treatment options, including efficacy and risks.
TABLE
Treatment options for keloids
| Treatment | Anticipated effects | Dosing and frequency | Efficacy in reducing keloid size | Adverse effects | SOR |
|---|---|---|---|---|---|
| Hygienic relief: washing & drying | Relief of pruritus, pain, general discomfort | As needed | N/A | Minimal | C |
| Antihistamines | Relief of pruritus, pain, burning sensation9 | As needed | N/A | Minimal | C |
| Corticosteroid injections | Reduction in keloid size, pruritus10 | Injections given every 4-8 wk for several months10 | >80% report moderate to marked regression10 | Local or systemic infection and allergy or anaphylaxis10 | B |
| Surgical excision | Temporary reduction in keloid size11 | Not successful as monotherapy; combine with alternative therapies as needed11 | Temporary; keloids always recur after excision11 | Chance of infection, excessive bleeding, or injury to adjacent tissues11 | C |
| Pressure therapy | Reduction in keloid size3,12 | Pressure of 25-40 mm Hg for 23-24 h/d over several months3,12 | 60%-80% of patients report at least partial improvement3 | Minimal; rarely, skin thinning and redness3,12 | B |
| Radiation therapy | Reduction in keloid size3 | 10-20 Gy fractionated over several weeks5 | Up to 94% of patients report improvement, but recurrence is common3 | Minimal; theoretical risk of malignancy13 | B |
| Silicone occlusive dressings | Reduction in pain, pruritus, and keloid size1,12,14 | Applied topically for 12-24 h/d for 18 mo1,12,14 | 68%-86% of patients report improvement in keloid texture, color, and size14; may be useful as a preventive measure14 | Skin breakdown, rash, pruritus12 | B |
| N/A, not applicable; SOR, strength of recommendation. | |||||
Offer symptomatic therapy routinely
Some patients find symptomatic relief through hygienic measures, such as regular washing and drying. Antihistamines can relieve symptoms of burning or pruritus,9 but are not expected to reduce keloid size.
Use corticosteroids for first-line treatment
Corticosteroids are the most widely used therapy for keloids.3 They decrease keloid bulking by inhibiting collagen synthesis1 and stimulate tissue collagenases and collagen degradation.5 Commonly used in the office setting are intralesional injections of triamcinolone acetonide, a potent anti-inflammatory and highly atrophogenic agent.
Administer injections every 4 to 8 weeks until clinical improvement (usually requiring several months) or prohibitive adverse effects occur. A general dosing guideline is about 0.1 to 0.2 mL of corticosteroid for every square centimeter of keloid tissue. Injecting higher doses can lead to accretions or deposits beneath the skin that might need to be unroofed. Additionally, excess corticosteroid can cause an atrophic contour deformity in the adjacent subcutaneous tissue. FIGURE 2 details steroid injection procedures and follow-up based on the author’s (SPD) experience.
FIGURE 2
A 5-step procedure for injecting keloids with corticosteroids*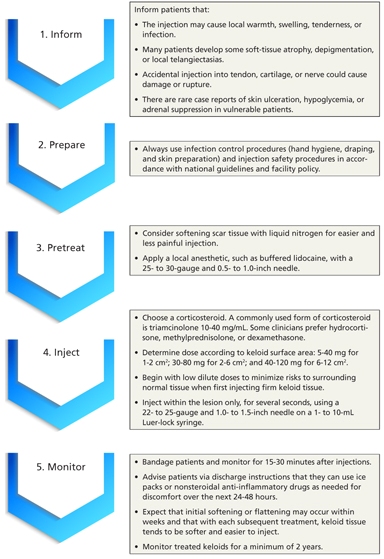
*Based on the author’s (SPD) experience.
Contraindications to injections include local or systemic infection and known allergy or anaphylactic reaction to corticosteroids. Although injecting keloids can be difficult initially, the tissue tends to soften and become easier to inject with each successive treatment. Some clinicians advocate cryotherapy to soften the keloid before giving injections. Large trials, in which more than 80% of patients had moderate to marked keloid regression,10 have demonstrated the efficacy of this technique in reducing keloid size and itching.
Surgery alone is ineffective
The oldest remedy, simple scalpel excision of keloidal tissue, invariably results in regrowth, because the aberrant wound healing process is not remedied.11 Although surgical excision is a poor monotherapy, it may be useful in combination with other modalities. Repairs using meticulous atraumatic surgical techniques with minimal wound tension can lessen the risk of keloid recurrence. Absorbable monofilament sutures with a subcuticular stitch help to minimize further epidermal damage.6
Pressure is useful in certain cases
Applying pressure is a noninvasive method that produces initial tissue thinning and pliability, with 60% to 80% of patients reporting at least partial improvement.3 Pressure reduces keloids by decreasing tissue metabolism, so long-term therapy is required, with application of pressure 23 to 24 hours daily over several months.12 Pressure of 25 to 40 mm Hg is needed to exceed capillary pressure without damaging peripheral circulation.3