3 alternatives to standard varicose vein treatment






For many patients with chronic venous insufficiency, thermal and chemical ablation could mean less pain and a speedier recovery.
TABLE
Endovenous thermal ablation vs standard surgery
| Outcomes | |||||
|---|---|---|---|---|---|
| Study | Type | Modalities studied | Follow-up | Return to work | Pain |
| Rautio et al20 | RCT | RFA vs stripping | 8 weeks | Earlier with RFA | Less with RFA |
| Lurie et al21 | RCT | RFA vs stripping | 2 years | N/A | Less with RFA |
| Hinchcliffe et al22 | RCT | RFA vs stripping | 1 year | N/A | Less with RFA |
| Darwood et al23 | RCT | ELT vs stripping | 3 months | Earlier with ELT | Less with ELT |
| ELT, endovenous laser treatment; NA, not available; RCT, randomized controlled trial; RFA, radiofrequency ablation. | |||||
FIGURE 1
Endovenous laser treatment
In preparation for thermal ablation, the physician (A) places a laser catheter tip into the vein and (B) injects perivenous tumescent anesthesia, guided by duplex ultrasound. The laser tip shown here (C) is in the region of the saphenofemoral junction.
Not for every patient
Despite the usefulness of these minimally invasive procedures, RFA and ELT are not always possible. Veins that are tortuous, too small, or too close to the surface of the skin are not well suited for thermal ablation; in some cases, chemical ablation, discussed below, is the only option. However, some conditions—including pregnancy, active DVT, poor health status with limited mobility, and severe peripheral vascular disease—are contraindications for both thermal and chemical ablation.24
Thermal won’t work? Consider chemical ablation
Endovenous chemoablation (ECA), like thermal ablation, is performed on an outpatient basis without sedation. Hypertonic saline, an osmotic agent, has been used for decades in treating small-caliber varicose veins, or “spider veins.” Detergenttype sclerosants, which we’ll discuss here, are now widely used to treat larger veins, including the great and small saphenous vein trunks and their affected tributaries.
Better suited for tortuous veins. Patients who have had prior stripping often have branches that are too tortuous to access with thermal ablation. In such cases, ECA is the only option. Those who have never undergone vein stripping often need a combination of thermal and chemical ablation, as well, with ECA reserved for saphenous veins that are inaccessible by RFA or laser.
Foamed sclerosants allow visualization. When mixed through a 3-way stopcock with an inert gas such as room air or carbon dioxide, the detergent-type sclerosants produce a micro-foamed preparation that is echogenic, and allows direct visualization with ultrasound (FIGURE 2). The foam displaces blood from within the vein and promotes contact with the venous endothelium, and intense vasospasm results. The sclerosant foam mixture, which makes it possible to watch the effect (and extent) of the foam as it disperses throughout the target vessel, has enhanced the treatment of larger viscosities.25-26 Pretreatment venous ultrasound mapping—a process in which the patient stands upright while compression is applied to the saphenous veins and their tributaries to test the valves for normal flow—combined with realtime duplex imaging, minimizes the chance of arterial injection, extravasation, and tissue necrosis.25
Serious adverse effects are rare. Hemosiderin hyperpigmentation and pain at the injection site are among the most common side effects of ultrasound-guided sclerotherapy. Serious adverse events, including anaphylaxis, DVT/pulmonary embolus, cutaneous necrosis, transient ischemic attack, and arterial injection, are rare.27
To date, there is only 1 published prospective, randomized study that directly compares foam sclerotherapy with stripping/ligation surgery. The researchers found the results of both treatments to be comparable, but reported that surgery was more expensive than foam sclerotherapy and produced less improvement in quality of life.28 A meta-analysis of treatment for 12,000 limbs concluded that foam sclerotherapy and EVTA were as effective as surgical stripping.29 There are no prospective, randomized studies comparing foam sclerotherapy with thermal ablation.
FIGURE 2
Endovenous chemoablation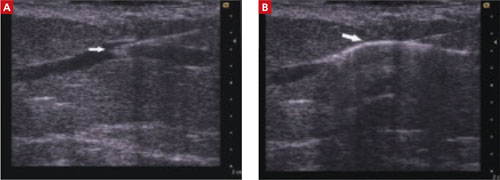
ECA is also conducted under ultrasound guidance: The image at left (A) shows the needle tip inside a refluxing saphenous tributary vein; in the image at right (B), the arrow points to the vein injected with foamed sclerosant.
Advising Kevin M.: What’s his best bet?
You’ve talked to your patient in the past about vein stripping, but he’s been reluctant to undergo surgery. When you describe the minimally invasive approaches to chronic venous insufficiency with him, however, he asks to see a specialist—and to undergo ultrasound mapping.
You give him a prescription for graduated compression stockings for immediate use and a referral to a phlebologist. Soon after, you receive a report from the specialist, indicating that your patient had a combination of ELT of the refluxing left great saphenous vein and subsequent ultrasound-guided ECA of the saphenous tributaries.
The next time you see Kevin, he reports that his leg no longer aches—and you can see that the bulging, tortuous varicosities and swelling have improved significantly.