Abnormal uterine bleeding: Avoid the rush to hysterectomy






Patients with heavy bleeding may think hysterectomy is their only recourse, but research supports other alternatives.
What else do you observe? When evaluating patients with abnormal uterine bleeding, don’t let the obvious focus on the gynecologic organs cause you to overlook other possibly significant findings. Look for acanthosis nigrican and an elevated body mass index (BMI), signs of PCOS, and also check for evidence of hyperthyroidism or galactorrhea. The bimanual exam should determine if the patient has an enlarged uterus, suggesting fibroids or adenomyosis.
TABLE 1
Abnormal uterine bleeding: 4 categories, many causes
| CATEGORY | MOST COMMON TYPE OF BLEEDING | SELECTED CAUSES |
|---|---|---|
| Bleeding associated with uterine pathology | Heavy bleeding, regular cycle (menorrhagia) | Endometrial polyps Adenomyosis Uterine fibroids Endometrial hyperplasia Uterine cancer |
| Dysfunctional uterine bleeding (DUB) without anatomic abnormalities | Heavy bleeding, irregular cycle (menometrorrhagia) | Polycystic ovarian syndrome Hypothalamic dysfunction
|
| Bleeding with a systemic illness | Usually menometrorrhagia | Thyroid dysfunction Elevated prolactin levels Liver or renal disease Coagulopathy Leukemia |
| Iatrogenic bleeding | Usually menometrorrhagia | Oral contraceptives Depot medroxyprogesterone acetate Postmenopausal hormone therapy Anticoagulants Herbal supplements |
Refer for a look inside the uterus
Patients with a pelvic exam that is inconclusive or suggests an enlarged uterus will likely benefit from referral for transvaginal sonography. This procedure is considered by many to be the test of choice for abnormal uterine bleeding.6 Saline infusion vaginal sonography, however, is considered a more sensitive test by some authorities.7 In saline infusion sonography, the clinician infuses a small amount of sterile saline into the uterus via a small catheter, which distends the normally compressed uterine walls and allows visualization of any endometrial cavity abnormalities, such as polyps or fibroids (FIGURE).
Office or outpatient hysteroscopy can also help visualize the endometrial cavity to diagnose cavity defects. Although hysteroscopy is an excellent and usually well-tolerated technique for visualizing the endometrial cavity, it cannot visualize the myometrium or ovaries as saline infusion sonography can. (TABLE 2) details the pros and cons of these diagnostic procedures.
FIGURE
What a difference saline can make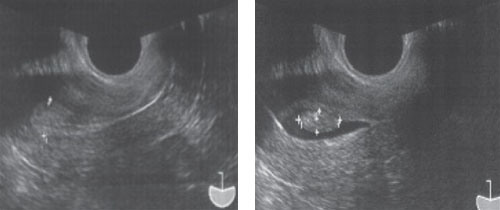
Routine transvaginal sonography shows the endometrium (calipers) without apparent abnormality. A previously undiagnosed endometrial polyp (calipers) in the same patient, revealed after saline infusion.
TABLE 2
Diagnostic studies: The pros, the cons
| STUDY | BENEFITS | POTENTIAL DRAWBACKS |
|---|---|---|
| Transvaginal sonography |
| May miss small or flaccid lesions (polyps) |
| Saline infusion vaginal sonography |
|
|
| Hysteroscopy |
|
|
What’s to be done?
In many cases clinicians can direct a plan of care on the basis of an accurate diagnosis. For example, patients with endometrial polyps or submucous uterine fibroids will benefit from referral to a gynecologist for outpatient surgical intervention. Otherwise, a variety of medical or minimally invasive surgical options are available.
Patients unaware of other options may come in asking about a hysterectomy, the second most common surgical procedure in the United States.8 Although this procedure is the definitive treatment for abnormal uterine bleeding, it carries the risk of surgical bleeding, ureteral or intestinal damage, incision breakdown, venous thromboembolism, and other intra- and postoperative problems.
While it is certainly appropriate to counsel the patient that hysterectomy is an option, there are many other options to consider. We now have a number of randomized trials that provide evidence-based guidance for the management of chronic abnormal uterine bleeding without hysterectomy (TABLE 3). These options can allow the patient to avoid the risks of major surgery and return to work and normal activities more rapidly.
TABLE 3
Beyond hysterectomy: Other treatment options to consider
| TREATMENT | COMMON REGIMENS | SOR | COMMENTS |
|---|---|---|---|
| Combined oral contraceptives9,12 | Cyclic or daily | A, B |
|
| Cyclic progestins9 |
| A | Side effects include spotting, weight gain, nausea, edema, and exacerbation of depression |
| NSAIDs14 | Mefenamic acid (Ponstel) 500 mg orally TID during menses; ibuprofen 800 mg orally TID during menses | A |
|
| Levonorgestrel IUS9,10 | Device provides 20 mcg/24 hours continuously for 5 years | A |
|
| Global endometrial ablation15,16 | Office or outpatient procedure | A |
|
| IUS, intrauterine system; NSAID, nonsteroidal anti-inflammatory drug. | |||
| Strength of recommendation (SOR) A. Good-quality patient-oriented evidence | |||