
Excluding deep vein thrombosis safely in primary care






Validation study of a simple diagnostic rule.
The FIGURE displays the graph of the ROC curve of the rule. The area under the ROC curve was 0.75 (95% CI, 0.70–0.79).
In the validation population, 112 patients (21%) fell in the “very low risk” group. Application of the rule could thus reduce the number of referrals by 21% in the validation set (TABLE 2). None of these patients had DVT (TABLE 2). Accordingly, sensitivity of the rule at the threshold of ≤3 in the validation population was 100% with a corresponding specificity of 25.7%. The predictive value of a negative test result was 100%, and the negative likelihood ratio 0 (TABLE 2). With increasing rule scores, the probability of having DVT rises. Besides, if the threshold of not referring a patient would be increased, sensitivity decreases and specificity increases (TABLE 2).
The complete case analysis revealed the same sensitivity, specificity, and negative likelihood ratio as the analysis on the imputed data—ie, no DVT cases in the very low risk group. All presented results are derived from the analysis of the imputed data set.
FIGURE
Receiver operator characteristic curve of the primary care rule for DVT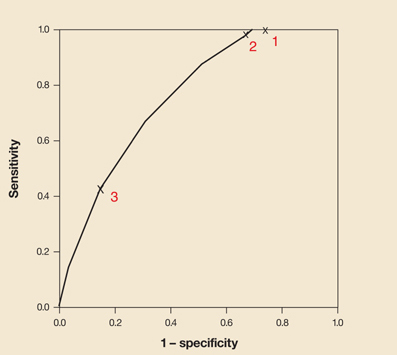
Points on the line correspond to the thresholds as displayed in Table 2. The values 1, 2 and 3 represent the sensitivities and specificities when applying a threshold of≤3, 6, and 9, respectively.
Discussion
To our knowledge, this diagnostic rule is the first for safely excluding DVT in primary care patients. Studies applying DVT rules in other settings have reported percentages of missed DVT cases similar to those in our study.16-20 Of these rules, the one developed by Wells and colleagues (Wells rule) is the best known.21-23
The Wells rule was derived and validated from data of 593 consecutively referred secondary care outpatients suspected of having DVT. In the Wells rule, 8 specific items from patient history and physical examination were weighted with 1 point (each item, if present, thus increased the likelihood of DVT equally) and a ninth item (another diagnosis just as likely or more likely to explain the presented symptoms and signs) was weighted –2 points (decreasing the likelihood of DVT). Accordingly, a sum of the scores given the 9 diagnostic items could result in a final tally from –2 to +8.
Wells et al initially presented their rule as a tool to exclude DVT if the score was 0 or lower (very low risk of DVT).21,22 In a more recent paper they updated their rule by adding the D-dimer test result and defined patients to be at very low risk with a score of 1 or less and a normal D-dimer test result.20 In secondary care, this rule yields good diagnostic accuracy in safely excluding DVT.
Uniqueness of our rule in primary care. In a recent study we showed that when testing the initial and updated Wells rule in primary care patients suspected of DVT, an unacceptably high percentage of patients in the “very low risk” group still had DVT: >12% for the initial rule and still >2% for the updated rule combined with D-dimer test.24 We repeated this analysis in the current cohort of primary care patients suspected of having DVT, which yielded similar results (data not shown). The decreased accuracy of the Wells rule in primary care can probably be ascribed to the differences in spectrum of patients between secondary and primary care.24
Value of the validation study. Many prediction rules are developed and recommended for use in new patients without external validation. It is well known that they yield risk estimations that are too optimistic when applied to other data. Our study quantified the generalizability of our simple rule to safely exclude deep venous thrombosis in primary care.4 Safely excluding a disease requires a high sensitivity and a high negative predictive value. The sensitivity (100%) and the negative predictive value (100%) in the new patient sample were the same as in the derivation study.
The threshold works. The derivation and validation studies both demonstrated that almost one quarter of the patients suspected of having DVT (23% and 21%, respectively) were at very low risk (score≤3) and could safely remain in primary care (0.7% and 0% missed DVT cases, respectively). Since all 112 individuals in the validation study with a very low risk at DVT were free of DVT, sensitivity and negative predictive value of the rule in the validation study were both 100% (both 99.3% in the derivation study), with a negative likelihood ratio of 0 (TABLE 2). Hence, we conclude that the developed rule seems a safe tool to use for excluding DVT in primary care.
