Self-doctoring: A qualitative study of physicians with cancer






Discussion
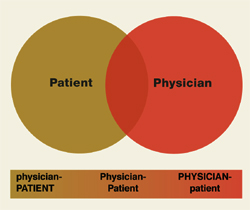
The attitudes and experiences of the study participants paralleled the medical literature: all but 1 recommended against self-doctoring, yet almost all were able to identify situations in which they did doctor themselves. Our findings show that participants’ health care-seeking strategies can be identified along a continuum ranging between the roles of physician and patient ( Figure 1 ). Whereas previous literature on physician-patients has characterized their situation as “role-reversal,”16,19,27 our findings suggest that physicians assume both roles depending on circumstances, influenced by their desire for control and degree of trust.
Trusting health care may be particularly difficult for physician-patients.2,3,27 In our study, participants at the “physician” end of the continuum were reluctant to “let go” of control over care, especially care they did not trust. They valued the convenience and time saved when they did things themselves and felt less need for support from their professional caregivers. These physicians did not consciously set out to doctor themselves. Instead, they simply used the expertise and status of their physician role to take care of themselves in the same way they might take care of a patient.
At the “patient” end of the health care-seeking continuum, participants approached their own health care as they thought a patient should. They tended not to be as involved with the details of their care, felt less pressure to be an expert in their own illness, and wanted their doctor to play an active role in medical decisions. They frequently emphasized the importance of being able to trust their care to another person and letting go of the need to be in control of their care. They valued the relationships with their physicians and appreciated the support these relationships provided.
Negative experiences invariably changed participants’ attitudes and where they were identified on the continuum. Both roles included unanticipated pitfalls, particularly for participants who adhered rigidly to either end of the continuum.
This study had important limitations. We recruited only physician-patients with cancer from a single institution and our sample was skewed toward survivors and presumably toward individuals who were comfortable talking about their experiences. Moreover, we replied on a convenience sample of patient-physicians identified by their specialists. Thus, the transferability of out findings ma be limited. Finally, our data captured the perspective of only the “physician-patient”—we did not interview their physicians. Nonetheless, we believe this provides robust new insights into physicians self-doctoring behaviors in the face of a serious, life-threatening illness.
Our findings make sense of the apparent mismatch between expert recommendations and physicians’ stated beliefs on one side, and physicians’ reported activities on the other. Rather than warning physicians not to doctor themselves, we advocate trying to focus on what is important: obtaining and providing good care ( Table 3 ). These questions are derived from 1 or more participating physician-patients’ experiences. In this way, we hope that readers might benefit from our participants’ experiences.
TABLE 3
Questions for physicians to ask themselves when seeking health care
| Are you responding more like a patient or more like a physician? Why? |
| If you are responding more like a physician: |
| Is it out of habit or convenience? |
| Is it because you don’t trust your doctors or health system (or because they are untrustworthy)? |
| Are you using your role as physician to shield yourself from painful or overwhelming realities? |
| Was an error made, or were you not getting the care you thought necessary? |
| AND |
| Do you have, or can you get, the necessary expertise to deal with your illness? |
| Are you too emotionally involved to be objective (and how would you recognize this problem)? |
| Do you, at minimum, have a physician you can trust and collaborate with—one with whom you would feel comfortable being a patient? |
| Are you getting the psychosocial support that may help you? |
| Are your nonmedical needs (rest, recreation, time off, decreased responsibilities at work) being met? |
| Are you getting the care you would want a patient in your position to receive? |
| If you are responding more like a patient: |
| Is it because you want to be “a good patient”? |
| Is it because you want someone else to make your decisions for you? |
| AND |
| Do you trust your professional caregivers and health care system? (And is that trust well founded?) |
| Are you ignoring your medical training or instincts because you do not want to offend? |
| Are you getting the information that you need (especially informed consent)? |
| Are you getting the psychosocial support you need? |
| Are your nonmedical needs (rest, recreation, time off, decreased responsibilities at work) being met? |
| Is the care you are getting consistent with the standard of care? |
| If it is not, do you understand why? |
| Are you getting the respect you would want a patient in your position to receive? |
| In either case: Would you be better off responding more like a patient, or more like a physician? |
FIGURE 1
Physician-patient continuum