Outpatient treatment of heart failure






Suggested management of patients with heart failure
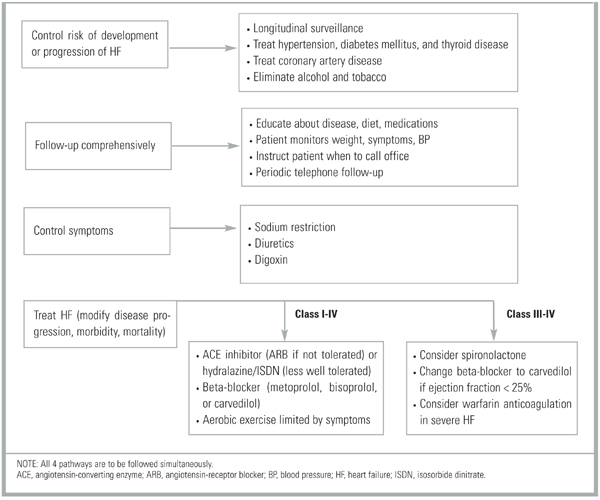
Although the optimal sequence of pharmacologic interventions for treating HF has not been examined in RCTs, recommendations can be made on the basis of existing evidence in HF management (Figure). This approach can be divided into 4 steps performed simultaneously: (1) control risks for the development and progression of HF (treat concomitant diseases); (2) HF treatment; (3) symptom control; (4) close follow-up.
Control risks. Risks for the development and worsening of HF should be addressed as described else-where.8 Steps include longitudinal surveillance; identification and treatment of hypertension, diabetes and thyroid diseases; management of atherosclerotic and coronary artery disease and myocardial ischemia; and the elimination of alcohol and tobacco use.
Heart failure treatment. All patients with HF should take a drug or a combination of drugs that affects the disease process. Drugs shown by the preponderance of evidence to decrease morbidity and mortality include ACE inhibitors, beta-blockers, and ARBs. For most HF patients, regardless of NYHA class, ACE inhibitors should be the initial baseline treatment because of their proven track record and the observation that most recent HF trials include patients who are already taking these medications. ARBs are similar in efficacy to ACE inhibitors and, therefore, are an adequate alternative when ACE inhibitors are not tolerated. Beta-blockers (metoprolol and bisoprolol) added to ACE inhibitors are also useful as a baseline treatment in most HF patients and may be especially useful in the case of tachydysrhythmias and in the postmyocardial infarction period.
For severe HF (NYHA III–IV), spironolactone and carvedilol are useful additions to baseline drug therapy. Carvedilol may be added if a beta-blocker is not currently used. If the patient is currently taking a beta-blocker, the drug should be discontinued before the patient is switched to carvedilol.
The hydralazine–nitrate combination has been proved effective, but tolerability and ease-of-use issues limit its usefulness. No data are available to support the use of nitrates other than isosorbide dinitrate. Nitrates may be useful, however, for concomitant chronic myocardial ischemia.
Patients with stable HF should be encouraged to begin and maintain a regular aerobic exercise program. The level of exercise can range from brief, symptom-limited exercise to moderate exercise (60% capacity) for 3 or more hours per week.
The use of antiplatelet therapy or the routine use of anticoagulation in patients with HF who are in sinus rhythm provides no benefit. Anticoagulation may be useful if the patient has severe HF or has a known mural thrombus. HF patients with atrial fibrillation should be considered for antiplatelet or anticoagulation therapy as described elsewhere.58
Short-acting CCBs may worsen HF. No data support the use of any CCB in the primary treatment of HF. Similarly, intermittent use of milrinone or dobutamine is not indicated.
Symptom control. The symptomatic treatment of HF includes the use of diuretics and dietary sodium restriction to control sodium levels and volume status. Symptom control should be accomplished along with the pharmacologic disease management outlined above.
The role of digoxin in the failing heart without dysrhythmias is unclear. Digoxin may be most useful in symptom control, as it reduces hospitalizations attributed to worsening HF. This benefit must be balanced against an increased risk of hospitalization caused by digoxin toxicity. Patients who are already taking digoxin should probably continue to do so. The role of digoxin in newly diagnosed HF patients is unknown.
Close follow-up. Comprehensive follow-up, with the patient as a more active participant and in which care is extended beyond the hospital or office to the home, is a key strategy in the long-term care of HF patients. This aspect of HF management should include educating patients about their disease process and their dietary and pharmacologic treatments; teaching them how to monitor their weight, symptoms, and blood pressure and to understand when to seek care; and following up periodically by telephone between scheduled office visits.
FIGURE
Management of adults with heart failure