Use of complementary therapies to treat the pain of osteoarthritis






Evidence shows that an integrative approach to therapy with complementary treatments improves patient outcomes.
Pharmacologic intervention is best begun with the least risky agent, at the lowest effective dose, for the shortest possible duration.12 For mild-to-moderate pain, the Osteoarthritis Research Society International recommends acetaminophen as initial therapy, given up to 4 g/d. If pain relief is insufficient, consider adding or switching to an oral or topical non-steroidal anti-inflammatory drug (NSAID), keeping in mind the possibility for gastrointestinal (GI) adverse effects with oral agents. When using an oral NSAID in patients at risk for GI effects, give a proton-pump inhibitor (PPI) as well. A topical NSAID or capsaicin may provide additional local pain relief.20
If pain remains inadequately controlled, or if a patient is intolerant to NSAIDs, a selective COX-2 inhibitor given alone or in
combination with acetaminophen may be an appropriate choice—provided the patient undergoes thorough evaluation for cardiovascular (CV) and GI risks.12,21 For those with GI risks taking a COX-2 inhibitor, give either misoprostol or a PPI concomitantly. Monitor those with CV risks closely.
When OA pain is severe or unresponsive to the previous medications, alternative agents include tramadol with or without acetaminophen, or opioid analgesics. In either instance, start at the lowest possible dosage (adjusted, as needed, for renal or hepatic impairment) and then titrate upward slowly to minimize adverse effects.9,12
Evidence-based complementary treatment options for OA
In its executive guidelines for US hospitals, the Joint Commission clearly states that institutions seeking accreditation, or wishing to maintain it, must include in its options for treating chronic pain such complementary measures as massage, acupuncture, and mind-body therapy. The Joint Commission’s basis for mandating an integrative approach to pain control is the growing body of clinical evidence supporting the efficacy of complementary treatments. In addition, many patients prefer nonpharmacologic options for personal reasons.
Hyaluronic acid. In a recently published meta-analysis of studies looking at intra-articular hyaluronic acid (IAHA) for knee OA pain, the authors reported therapeutic effectiveness beginning at 4 weeks, reaching a peak effect at 8 weeks, and exerting a residual effect still detectable at 24 weeks.22 Moreover, the peak effect of IAHA is greater than published effects for acetaminophen, NSAIDs, and COX-2 inhibitors.22 IAHA could be useful in combination with other therapies, and in certain clinical situations such as when patients are undecided about surgery. Other studies and meta-analyses of IAHA have yielded different results regarding length of efficacy.23,24
Acupuncture. While studies of acupuncture for OA have varied in quality and duration of effect, many show benefits. One meta-analysis found that patients who received acupuncture reported clinically relevant short- and long-term pain reduction and improved function compared with control patients who received usual care.25 In a study of
294 patients with OA of the knee, patients received 8 weeksof acupuncture, minimal acupuncture (superficial needling at nonacupuncture points), or no treatment. Based on the Western Ontario and McMasters Universities Osteoarthritis (WOMAC) questionnaire assessing pain, function, and stiffness due to OA, those who received acupuncture had significantly better scores than the other 2 groups. However, after 26 and 52 weeks, the differences between acupuncture and minimal acupuncture were no longer significant.26
In the largest study ever conducted on acupuncture for OA of the knee, 570 patients were randomly assigned to receive acupuncture, sham acupuncture, or education.27 At
26 weeks postintervention, based on the WOMAC function score those who underwent true acupuncture experienced significantly greater pain relief and functional improvement than those who received sham acupuncture or education only.
Mindfulness-Based Stress Reduction (MBSR), pioneered by Jon Kabat-Zinn, PhD, uses mindfulness meditation to alleviate chronic pain. First reported in a 1982 study, 88% of enrolled patients with chronic pain of 6 months to 48 years’ duration who were trained in stress reduction using mindfulness meditation perceived a decrease in pain of at least 50%.28 This method of focusing on the mind and body does not simply “distract” patients from their pain but achieves measurable changes in how pain is perceived. With MBSR, pain reduction reported by patients was significantly greater than that achieved with morphine and other drugs.29 Brain scans show that, after MBSR, regions normally associated with processing painful stimuli become quiescent.29 MBSR has also been shown in imaging studies to increase gray matter concentrations in regions of the brain associated with learning and memory, regulation of emotion, and self-referential processing [Figure 2].30
| FIGURE 2: Gray matter is more concentrated for persons who meditate compared with nonmeditators. |
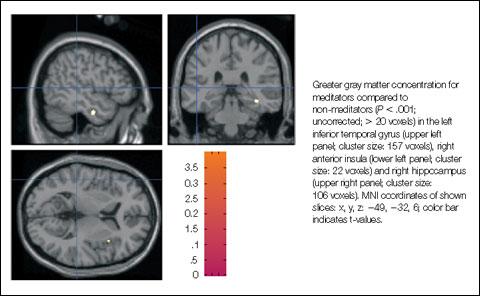
| Source: Holzel BK, et al. Soc Cogn Affect Neurosci. 2008;3:55-61 |
A 2004 meta-analysis of 20 reports on mindfulness meditation that met study criteria included patients with anxiety, cancer diagnoses, chronic pain, coronary artery disease, depression, fibromyalgia, obesity and binge eating disorders, and psychiatric disorders. The analysis found a relatively consistent and strong effect, suggesting that mindfulness training may enhance the ability to cope with distress and disability and the sense of physical well-being.31