Hand compression neuropathy: An assessment guide






When a patient presents with pain or paresthesias of the hand and fingers, knowing what to ask, what to look for, and which tests to consider is essential.
Proceed with caution. Provocative testing with a pronated forearm and a flexed and ulnar-deviated wrist may exacerbate symptoms,12,42 and Finkelstein’s maneuver (isolated ulnar deviation at the wrist to elicit pain over the first dorsal wrist compartment) and Phalen’s test may elicit false-positive results. Upper motor neuron exams (ie, deep tendon reflexes) and Hoffman’s sign (reflexive flexion of the terminal phalanges of the thumb and index finger induced by flicking or tapping the distal phalanx of the long finger) should be symmetric to the contralateral extremity.
In patients with more than one compression injury, Spurling’s sign (neck extension and lateral rotation towards the affected extremity) may induce paresthesia when combined with axial compression, while the shoulder abduction test (shoulder 90° abduction, with external rotation) may diminish reported paresthesia. In those for whom Wartenberg’s syndrome is their only compression injury, however, these provocative maneuvers will be negative.
Anterior interosseous nerve syndrome
A rare clinical entity that affects the anterior interosseous innervated muscles in the forearm, anterior interosseous nerve syndrome (AINS)’s etiology is unclear. But it is likely related to a spontaneous neuritis rather than a compressive etiology.43 Paresis or paralysis of the flexor pollicis longus (FPL) and the flexor digitorum profundus (FDP) of the index and long finger is its hallmark, but patients may report vague forearm pain associated with weakness or absence of function.
Examination begins with a visual assessment and palpation of the forearm and hand for atrophy or a space-occupying lesion. Notably, sensory function of the hand should remain at baseline despite the motor dysfunction, as the anterior interosseous is purely a motor nerve.
Motor testing should focus on the median and anterior interosseous innervated muscles.
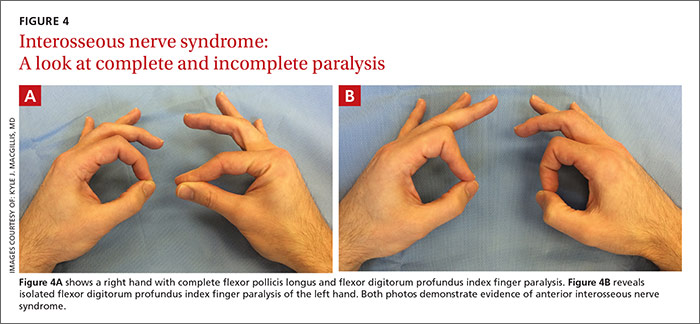
The FPL is tested by isolated thumb IPJ flexion and the Kiloh and Nevin sign—the inability to make an “OK” sign with the thumb and index finger.44 Assess pinch grasp with a maximally flexed thumb IPJ and distal IPJ of the index finger. Anterior interosseous nerve dysfunction results in a flattened pinch without IPJ or distal IPJ flexion, which increases the contact of the thumb and index finger pulp.45 In a series of 14 patients, researchers reported complete paralysis of FPL and FDP index finger in 5 patients, isolated paralysis of FPL in 7 patients, and isolated paralysis of FDP index and long fingers in 2 patients. None had isolated paralysis of the FDP long finger.46FIGURE 4 shows complete (A) and incomplete (B) paralysis.
Evaluation of AINS also includes assessment of FPL and FDP tendon integrity with passive tenodesis. The appearance of the hand at rest should reflect the natural digital cascade. In a completely relaxed or anesthetized hand, the forearm is placed in wrist supination and extension, allowing gravity to extend the wrist and placing the thumb MCPJ at 30° flexion, the index finger MCPJ at 40°, and the small finger MCPJ at 70°. The thumb IPJ should approximate the radial fingertip pulp of the index finger. The forearm is then pronated and flexed at the wrist, straightening the thumb MCPJ and producing a mild flexion cascade at the proximal and distal IPJ of the index, long, ring, and small fingers within 20° of full extension. This dynamic exercise is used to confirm that the patient has an intact tenodesis effect, thus excluding tendon lacerations or ruptures from the differential diagnosis. In one study, in 9 of 33 cases of partial or complete isolated index finger FPL or FDP, paralysis was initially diagnosed as tendon rupture.47
When to consider electrodiagnostic testing
Electrodiagnostic testing—a combination of electromyography and nerve conduction studies to assess the status of a peripheral nerve48—provides objective data that can help diagnose a challenging presentation, rule out a competing diagnosis, or clarify an atypical clinical picture or vague subjective history. This type of testing is also used to localize the entrapment site, identify a patient with polyneuropathy or brachial plexopathy, and assess the severity of nerve injury or presence of a double crush syndrome.49,50 Any patient with signs and symptoms of a compression neuropathy and supportive findings on physical exam should be referred for electrodiagnostic testing and/or to a surgeon specializing in treating these conditions.
CORRESPONDENCE
Kyle J. MacGillis, MD, University of Illinois at Chicago, Department of Orthopaedic Surgery, 835 South Wolcott Avenue, M/C 844, Chicago, IL 60612; kylemacgillis@gmail.com.