Patient with intractable nausea and vomiting






A chest x-ray—followed by further questioning about the patient’s medical history—revealed the cause of this woman’s symptoms.
Diagnosis: Achalasia
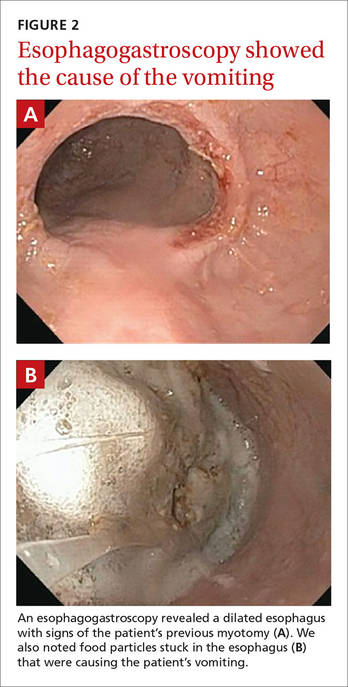
The radiologist who examined the x-ray noted a dilated esophagus (FIGURE 1, red arrows) with debris behind the heart shadow, which suggested achalasia. Upon further questioning, the patient reported a history of achalasia that had been treated with a myotomy 6 years ago. We performed an esophagogastroscopy, which showed a dilated esophagus with signs of the myotomy (FIGURE 2A), as well as food particles lodged in the esophagus (FIGURE 2B) that were causing the patient’s intractable vomiting.
Achalasia is a motor disorder of the esophagus smooth muscle in which the lower esophageal sphincter does not relax properly with swallowing, and the normal peristalsis of the esophagus body is replaced by abnormal contractions. Primary idiopathic achalasia is the most common form in the United States, but secondary forms caused by gastric carcinoma, lymphoma, or Chagas disease are also seen.1 The prevalence of achalasia is 1.6 per 100,000 in some populations.2 Symptoms can include dysphagia with solids and liquids, chest pain, and regurgitation.
A chest x-ray will show an absence of gastric air, and occasionally, as in this case, a tubular mass (the dilated esophagus) behind the heart and aorta. On fluoroscopy, the lower two-thirds of the esophagus does not have peristalsis and the terminal part has a bird beak appearance. Manometry will show normal or elevated pressure in the lower esophagus. Administration of cholinergic agonists will cause a marked increase in baseline pressure, as well as pain and regurgitation. Endoscopy can exclude secondary causes.