Headaches






Although most headache presentations to the ED are of benign etiology, there are several potentially life-threatening conditions for which the emergency physician should have a high index of suspicion based on symptoms. This special feature reviews migraine, thunderclap headache, and uncommon—but potentially serious and life-threatening—causes of headache.
The majority of patients with CVST have an underlying risk factor for thrombosis (eg, injury, infection). In addition, hypercoagulable states seem to be more commonly found in adults with CVST, whereas infection to the head and neck is a more common risk factor in children.1 Women in the peripartum period also seem to be particularly vulnerable.3,5
Symptoms and Diagnosis
Headache is the most common presenting symptom in patients with CVST, although focal neurologic deficits, seizures, and altered mental status may also be seen.3 The headache is usually described as worsening over days to weeks, but thunderclap headache may also be reported.2 In CVST, headache may be the only presenting symptom, making diagnosis difficult.6 A diagnosis of CVST should be considered in any patient presenting with headache in conjunction with cranial nerve 6 palsy or papilledema.
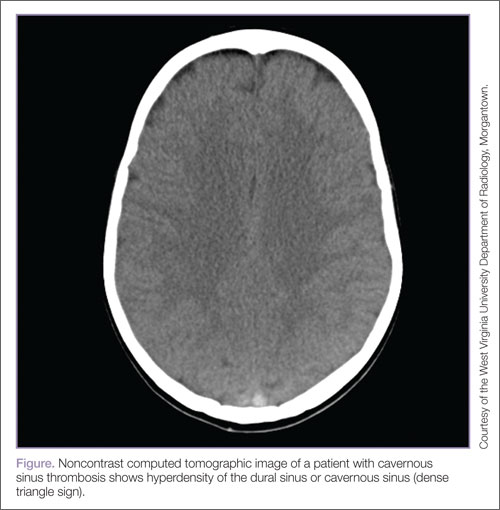
Workup of a suspected diagnosis of CVST can be challenging. A computed tomography (CT) scan of the brain with contrast may only diagnose 30% of cases.6 A noncontrast CT may be normal, but can show a hyperdensity of the dural sinus or cavernous sinus (dense triangle sign; Figure). Computed tomographic venography and magnetic resonance venography have much higher sensitivities in making the diagnosis.6 In addition to imaging studies, D-dimer elevation will be seen in most patients with this diagnosis, but a normal D-dimer may not exclude the presence of disease.4,7 Anticoagulation is considered first-line treatment even if an intracranial hemorrhage is present as a complication of the CVST.2,7 There may be a role for thrombolytic therapies in patients that clinically deteriorate despite anticoagulation.7
Occipital Neuralgia
Occipital neuralgia is characterized by a paroxysmal, lancinating pain over the area of the greater occipital nerve. It is typically associated with tenderness to palpation and may be described as a dysethesia or hypoesthesia.8,9 In occipital neuralgia, the pain originates in the suboccipital area of the head and radiates to the vertex. Although the exact etiology of the nerve irritation may be unknown, it is hypothesized that the cause could be vascular, muscular, osteogenic, or neurogenic.10 In addition to headache, patients may report blurry vision, orbital pain, nausea, dizziness, tinnitus, and nasal congestion.10 The true epidemiology of occipital neuralgia is unknown, as there are no clear diagnostic criteria or consensus on its definition.11 The pain may be spontaneous or provoked by exposure to cold or certain movements of the neck; it may be elicited by tapping on the occipital nerves (Tinel’s sign). The diagnosis is confirmed when the patient reports transient relief of pain after an occipital anesthetic block.11,12
Short-Lasting Unilateral Neuralgiform Headache Attacks With Conjunctival Injection and Tearing
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing is a syndrome characterized by brief frequent attacks of stabbing pain in and around the eye, and associated tearing. Attacks may occur a few times a day, but often hundreds of times a day, lasting anywhere from seconds to several minutes.13 The short duration and higher frequency of attacks are useful criteria for differentiating SUNCT from cluster headache. Since SUNCT has some association with pituitary tumors, referral for outpatient magnetic resonance imaging is a reasonable recommendation.14 Small studies have shown some promise in improving symptoms with treatment with carbamazepine, gabapentin, and lamotrigine15,16 Steroids have been used with some success in temporarily aborting symptoms of this syndrome, which may be useful in treating patients presenting to the ED.17,18
Giant Cell Arteritis
Giant cell arteritis, also known as temporal arteritis or cranial arteritis, can be a cause for significant morbidity in those affected, with permanent visual loss being the most important complication. The typical presentation is new-onset focal headache in a patient older than age 50 years. The headache may be accompanied by a wide range of visual symptoms. In fact, visual symptoms with or without headache may be the presenting complaint, requiring clinician vigilance to seek out this diagnosis. Other historical features may include jaw claudication, fever, and symptoms of polymyalgia rheumatica.
The clinical presentation of polymyalgia rheumatica, which is present in up to half of patients, is one of proximal symmetric muscle and joint aches, accompanied by constitutional symptoms. Physical examination may be very nonspecific, but the temporal arteries may be tender with diminished pulses. The most useful laboratory finding is an elevated erythrocyte sedimentation rate, which is classically >50, though there have been documented cases with lower levels. An elevated C-reactive protein may be more predictive of the presence of GCA, but more research is needed in this area.19 A complete blood count may reveal a normochromic, microcytic anemia.
The pathophysiology of GCA involves inflammation of larger arteries, usually of the upper body and cranium. A wide range of vascular complications are possible, including ischemia, aneurysm, and dissection to affected vascular territories. The most common serious complication of GCA is permanent visual loss due to ischemic retinopathy. Ophthalmic involvement occurs in 26% of patients with permanent visual loss in 7% to 14%.