Acute Limb Arterial Ischemia





Physical Examination
On physical examination, the EP should pay particular attention to both the external appearance and temperature of the skin of the patient’s affected extremity. The presence or absence of peripheral pulses is an important feature when assessing for ALI; however, the presence of peripheral pulses does not exclude ALI from the differential.
Precise evaluation of sensation is important to attempt to quantify the extent of injury, localize a possible obstruction, and differentiate ALI from other possible causes of sensation deficits. Though not referenced in the six Ps, the patient’s limb may also appear mottled or marbled. Embolic phenomena occur at sites of vascular bifurcation. In a patient with aortic embolism, femoral pulses will be absent with bilateral mottling and paralysis of the lower extremities. Iliac artery embolism will produce the same symptoms, except unilateral. Femoral artery embolism will yield coolness and mottling distal to the inguinal ligament. Similarly, popliteal artery embolism will produce those same findings, except distal to the knee with preserved femoral pulses.
Diagnosis and Evaluation
After the history and physical examination are completed, further diagnostic methodologies should be considered, including laboratory evaluation and additional imaging studies.
Imaging Studies
Doppler ultrasound examination to assess for pulses on the affected limb should be performed immediately. Bedside continuous-wave Doppler may be used to differentiate arterial vs venous signal.6,14-16 An ankle brachial index may be calculated through either direct auscultation of pulses or Doppler signal. A ratio of less than 0.9 is suggestive of ischemia, while a ratio of less than 0.5 is considered critical ischemia.2
Laboratory Evaluation
Laboratory evaluation of hematocrit, coagulation studies, renal function, electrolyte levels, lactate, and creatinine kinase should be completed.1,5 An electrocardiogram and bedside/formal echocardiogram may be considered if embolism is suspected.1,6,17
Imaging
Angiography is currently the gold standard imaging modality to diagnose ALI.16 However, other imaging modalities exist that expose the patient to less radiation and are generally preferred by patients.18 Duplex ultrasonography is the least invasive imaging modality, with a reported sensitivity of 88% and specificity of 96% for the detection of greater than 50% stenosis.6,19 Contrast-enhanced magnetic resonance angiography (MRA) of the lower extremity is also relatively noninvasive, but is more limited in its application. It carries a reported sensitivity of 95% and a specificity of 97% for detection of stenosis of greater than 50%.6,19 An MRA without contrast may be considered for patients with an estimated glomerular filtration rate of less than 30 mL/min/1.73 m2 and who are not on dialysis, but the diagnostic efficacy is reduced.16 Finally, the sensitivity and specificity of computed tomography angiography (CTA) to detect aortoiliac stenosis of greater than 50% is 96% and 98% respectively.6,18,19 Other studies demonstrated similar results for other arterial locations in the lower extremities.18,19 A principal advantage of CTA is that direct visualization of calcifications, clips, stents, and prior bypasses is possible without the limitations of MRA.16 The American College of Radiology (ACR) lists ultrasound duplex Doppler and noncontrast MRA of the lower extremity as “may be appropriate.”16 In contrast, the ACR classifies MRA with contrast, CTA with contrast, and angiography of the lower extremity as “usually appropriate.”16 Selecting the optimal imaging study for a patient may require involvement of a facility’s radiology department and/or a vascular surgeon.14,15
Management in the ED
Even before the definitive diagnosis of ALI is made, steps can be taken to minimize and/or slow progression of injury. Placing the affected limb in a dependent position and providing intravenous (IV) fluid hydration will maximize perfusion.1,3,5 Even with consideration of the diagnostic modalities previously described, ALI is often considered a clinical diagnosis. Since time is critical, early consultation with vascular surgery services is imperative if ALI is suspected.
Intravenous Fluid Therapy
Suspected ALI should be treated in the ED with an IV heparin bolus, followed by constant IV infusion. Heparin prevents proximal and distal propagation of the thrombus.1,3,5,6,15,17,20 Additionally, it helps maintain the microcirculation surrounding the affected area.6 A heparin bolus dose of 100 U/kg followed by a continuous infusion of heparin 1,000 U/h is the recommended standard.1,3,5,6,15 A goal partial thromboplastin time of 60 to 100 seconds, or an international normalized ratio of 2 to 3 is desirable.8,21
Staging: The Rutherford Classification System
Once immediate therapies are started, the stage of PAD should be determined using the Rutherford classification system in collaboration with vascular surgery services; this will further guide treatment and disposition.
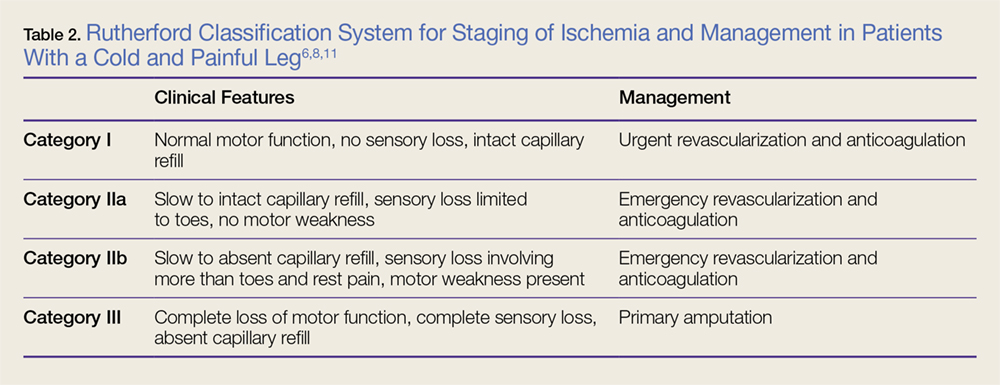
Category I. In category I ALI, the affected limb is considered viable and not immediately threatened.
Category IIa. The limb is considered to be marginally threatened and salvageable.
Category IIb. An ALI classified as a category IIb is the most urgent type in which the limb is immediately threatened.
Category III. The limb is classified as having irreversible damage.2,3,17,22
(See Table 2 for a more detailed summary of the Rutherford classification system.)