Prednisone and Vardenafil Hydrochloride for Refractory Levamisole-Induced Vasculitis





Levamisole is an immunomodulatory drug that was previously used to treat various medical conditions, including parasitic infections, nephrotic syndrome, and colorectal cancer. Over the last few years, increasing amounts of levamisole have been used as an adulterant in cocaine. Levamisole-cut cocaine has become a concern because it is known to cause a necrotizing purpuric rash, autoantibody production, and life-threatening leukopenia. Mixed histologic findings of vasculitis and thrombosis are characteristic of levamisole-induced purpura. The recommended management of levamisole-induced vasculitis currently involves withdrawal of the culprit along with supportive treatment. We describe a patient with levamisole-induced vasculitis who continued to develop skin lesions despite self-reported cocaine cessation. Complete resolution of cutaneous disease occurred with the addition of oral prednisone and vardenafil hydrochloride, suggesting the possibility of a new treatment option in patients with refractory disease. In addition, we review the clinical presentation, disease course, diagnostic approach, laboratory findings, histology, and management of levamisole-induced vasculitis. The harmful effects of levamisole-cut cocaine are serious enough that public alerts have been issued to increase awareness. Clinicians should consider the possibility of levamisole exposure in cocaine users presenting with any combination of fever, neutropenia, and necrotic skin lesions, especially in acral areas including the ears.
Practice Points
- Levamisole is an immunomodulatory drug that, before being withdrawn from the US market in 2000, was previously used to treat various medical conditions.
- A majority of the cocaine in the United States is contaminated with levamisole, which is added as an adulterant or bulking agent.
- Levamisole-cut cocaine is a concern because it is associated with a life-threatening syndrome involving a necrotizing purpuric rash, autoantibody production, and leukopenia.
- Although treatment of levamisole toxicity is primarily supportive and includes cessation of levamisole-cut cocaine, a trial of prednisone and vardenafil hydrochloride can be considered for refractory levamisole-induced vasculopathy or for patients who continue to use the drug.
Case Report
A 49-year-old man with a history of polysubstance abuse presented with intermittent fevers and painful swollen ears as well as joint pain of 3 weeks’ duration. One week after the lesions developed on the ears, similar lesions were seen on the legs, arms, and trunk. He admitted to cocaine use 3 weeks prior to presentation when the symptoms began.
On physical examination, violaceous patches with necrotic bleeding edges and overlying black eschars were noted on the helices, antihelices, and ear lobules bilaterally (Figure 1). Retiform, purpuric to dark brown patches, some with signs of epidermal necrosis, were scattered on the arms, legs, and chest (Figure 2).
,

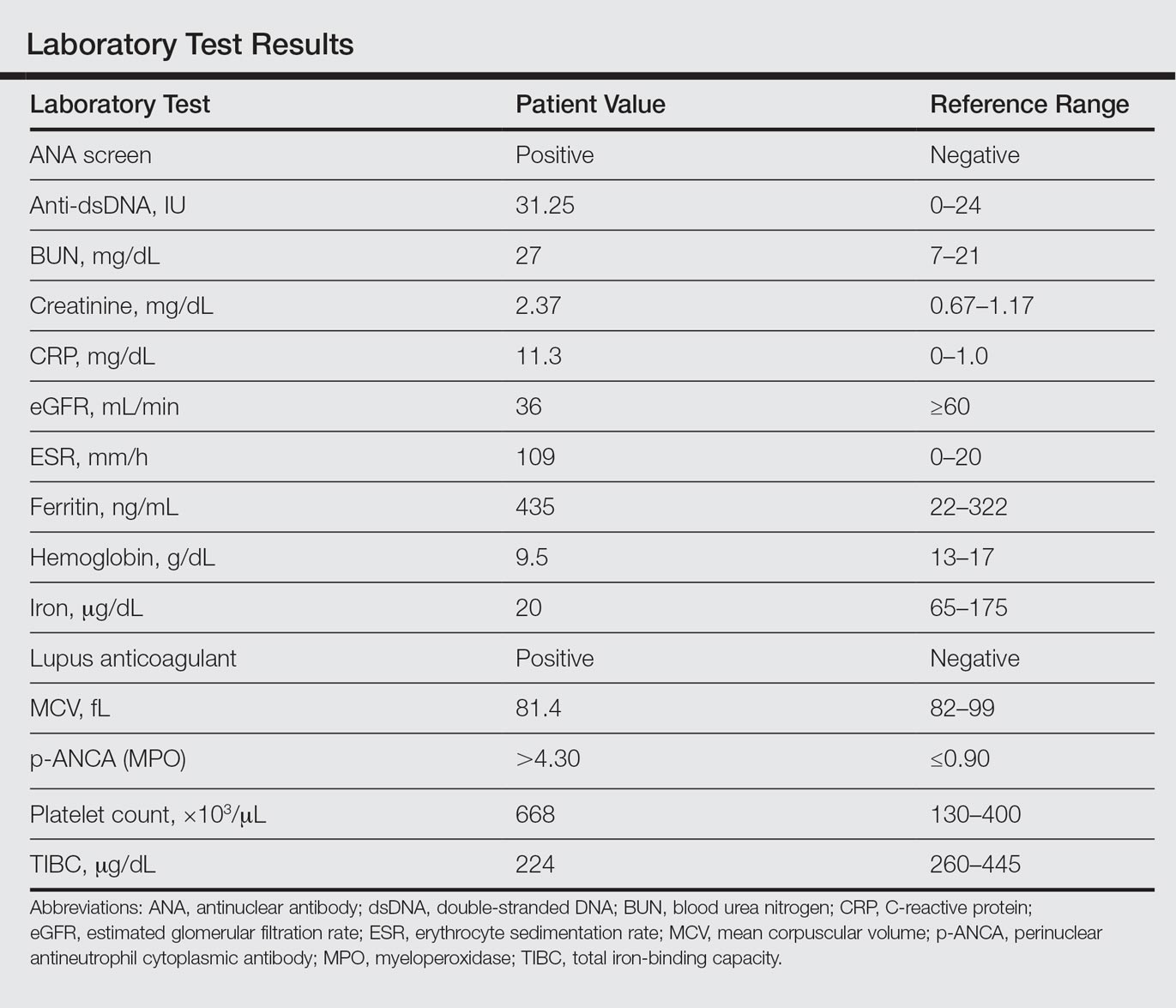
Laboratory examination revealed renal failure, anemia of chronic disease, and thrombocytosis (Table). The patient also screened positive for lupus anticoagulant and antinuclear antibodies and had elevated p-ANCA and anti–double-stranded DNA (Table). He also had an elevated sedimentation rate (109 mm/h [reference range, 0–20 mm/h]) and C-reactive protein level (11.3 mg/dL [reference range, 0–1.0 mg/dL])(Table). Urine toxicology was positive for cocaine.
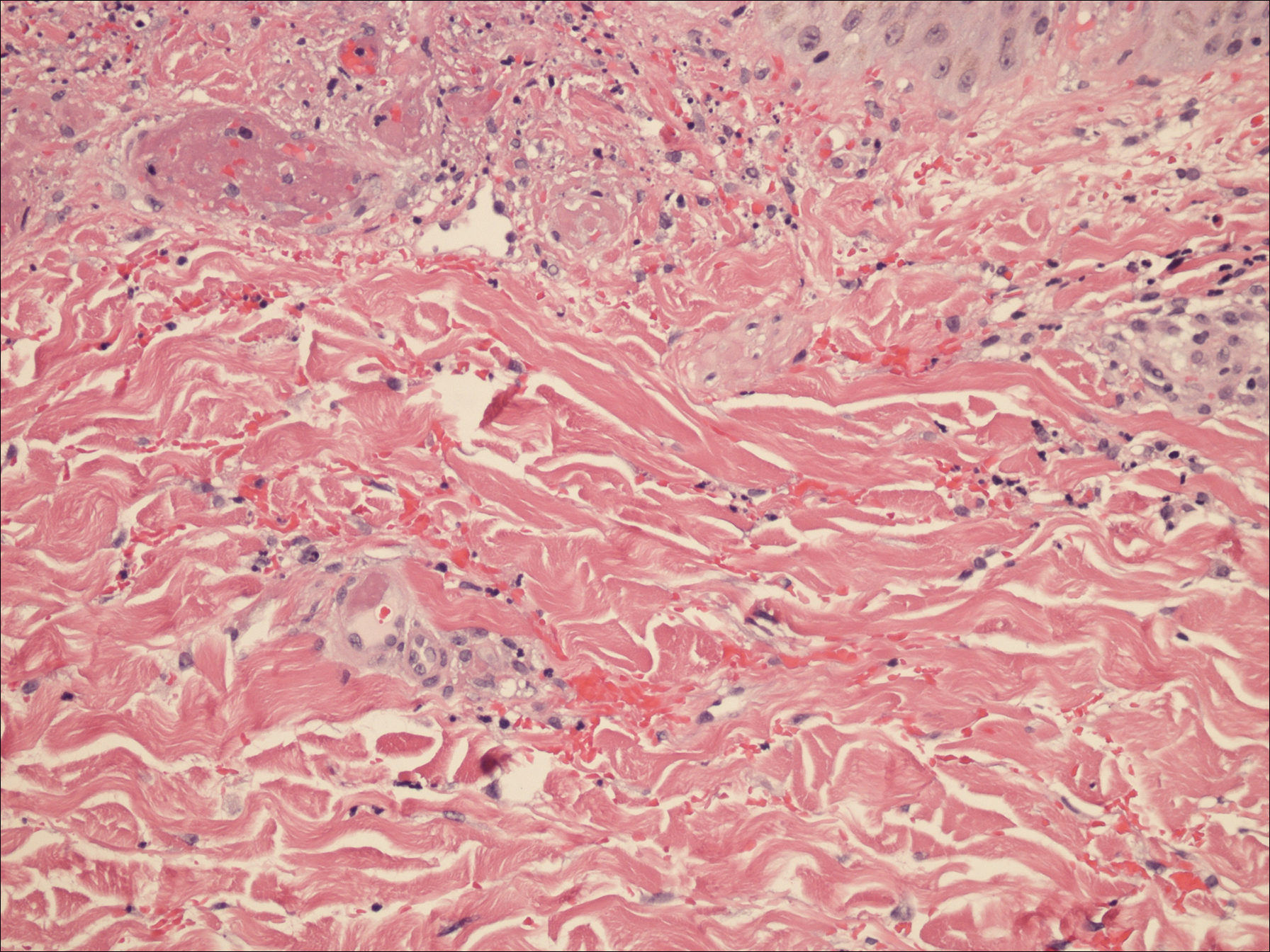
A punch biopsy of the left thigh was performed on the edge of a retiform purpuric patch. Histopathologic examination revealed epidermal necrosis with subjacent intraluminal vascular thrombi along with extravasated red blood cells and neutrophilic debris (leukocytoclasis) and fibrin in and around vessel walls, consistent with vasculitis (Figure 3).
The patient was admitted to the hospital for pain management and wound care. Despite cocaine cessation and oral prednisone taper, the lesions on the legs worsened over the next several weeks. His condition was further complicated by wound infections, nonhealing ulcers, and subjective fevers and chills requiring frequent hospitalization. The patient was managed by the dermatology department as an outpatient and in clinic between hospital visits. He was treated with antibiotics, ulcer debridement, compression wraps, and aspirin (81 mg once daily) with moderate improvement.
Ten weeks after the first visit, the patient returned with worsening and recurrent leg and ear lesions. He denied any cocaine use since the initial hospital admission; however, a toxicology screen was never obtained. It was decided that the patient would need additional treatment along with traditional trigger (cocaine) avoidance and wound care. Combined treatment with aspirin (81 mg once daily), oral prednisone (40 mg once daily), and vardenafil hydrochloride (20 mg twice weekly) was initiated. At the end of week 1, the patient began to exhibit signs of improvement, which continued over the next 4 weeks. He was then lost to follow-up.