Recurrent Pyogenic Granuloma With a Satellite Lesion





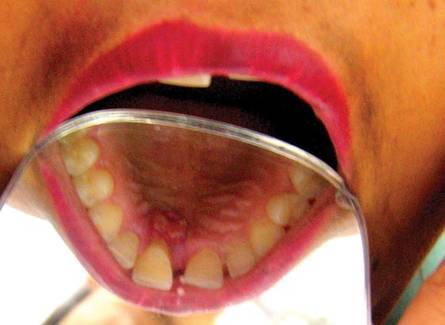
Pyogenic granuloma (PG) is a tumorlike growth of the oral mucosa or skin that is considered to be an exaggerated conditioned response to minor trauma. It usually is painless, bleeds easily, and is considered to be nonneoplastic in nature. Pyogenic granuloma predominantly occurs in the second decade of life, mostly among young adult females. Clinically, it is a smooth or lobulated exophytic lesion manifesting as small, red, erythematous papules on a pedunculated or sometimes sessile base that usually is hemorrhagic. We report the case of 30-year-old woman who presented with a PG in the anterior palatal region during pregnancy that recurred with a satellite lesion 1 year following surgical excision.
Practice Points
- Pyogenic granulomas (PGs) need to be excised down to the periosteum to decrease the chances of recurrence.
- Bleeding during excision of PGs is expected; therefore, aids to achieve hemostasis (eg, pressure packs, local hemostatic agents, electrocautery) should be available.
- The underlying cause for the lesion (ie, infection, trauma, irritation) has to be identified and treated to decrease the chances of recurrence.
| 
| |

| 
|
Comment
Pyogenic granuloma occurs in 0.2% to 9.6% of all pregnancies, highlighting the underlying hormonal changes in this patient population.1 In our patient, the initial lesion may have occurred due to the hormonal changes of pregnancy coupled with poor oral hygiene. Pyogenic granulomas that are excised during pregnancy are known to recur,9,10 and excision is only advised in this patient population if the lesion is causing disturbance in speech and mastication.9 In our patient, excision was performed following delivery because the initial lesion had not caused any disturbance in speech or mastication. Cases of larger PGs that do interfere with the patient’s speech and mastication may necessitate early excision prior to delivery.11 In our patient, thorough scaling and root planing around the involved teeth was done before excision of the lesion by the dentist. Despite taking these precautions to reduce the chances of recurrence, the lesion recurred 1 year following excision. Recurrence of PG after excision has been noted in up to 16% of cases.2 Profuse bleeding in our patient was encountered during excision of the initial lesion and was controlled using pressure packs and local hemostatic agents. It is possible that some small portions of the lesion were not excised due to the profuse bleeding. Bleeding during excision of PGs is expected; therefore, aids to achieve hemostasis (eg, pressure packs, local hemostatic agents, electrocautery) should be available. In spite of educating and motivating the patient to practice good oral hygiene, her oral hygiene status was poor, which could be an important factor in the recurrence of the lesion at the primary site and also may explain the occurrence of an additional growth/satellite lesion around the maxillary right canine. Occurrence of satellite lesions or additional lesions following excision of PG has been reported in the literature.12,13 However, the presence of additional lesions in the oral cavity or gingiva rarely has been reported.
Pyogenic granuloma is common on the gingiva, especially in pregnant women, and recurrence following excision is not rare. If causes of recurrence, such as chronic irritation factors, are resolved and excision is done with some amount of normal adjacent tissue down to the periosteum, chances of recurrence decrease.