Prostate Cancer





Prostate cancer incidence continues to rise by about 1% per year in the United States, with 192,000 new cases diagnosed in 2009. As increasing numbers of men follow recommendations to undergo PSA testing and digital rectal examination, the chances of detecting cancer still confined to the prostate—with optimal chances for a cure—also increase. How can clinicians help each patient make the best decisions regarding screening, biopsy, and (when required) treatment for the cancer that is second most common among US men?
In the absence of a family history of prostate cancer, it is recommended that men undergo annual DRE and PSA testing beginning at age 50.21,22 The American Urological Association13 recommends annual PSA testing beginning at age 40 for African-American men and other men with a positive family history of prostate cancer. The American Cancer Society23 recommends that these tests be offered annually to men who are 50 and older and who have at least a 10-year life expectancy.
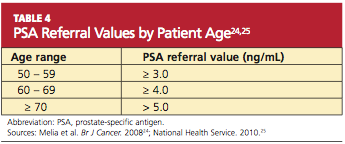
The serum PSA level alone does not automatically trigger a referral for a prostate biopsy (see Table 424,25). Other factors that should also be considered are family history, nonsymmetrical enlargement of the prostate, DRE findings of firmness, induration, or frank nodules, age, ethnicity, comorbidities, a history of previous negative prostate biopsy, and previous PSA levels. The patient should be involved in any decision regarding referral to another health care provider and the decision to perform biopsy.18
PSA levels are also used to monitor response to cancer treatments and to detect disease recurrence after treatment.2
Serum PSA Elevation
PSA is a prostate-specific marker, and elevations can be caused by prostate cancer or by benign conditions, such as BPH or infection. Malignant prostate tissue generates more PSA than does normal or hyperplastic tissue. The likelihood of finding cancer on a prostate biopsy increases as PSA values rise. Two PSA tests performed seven weeks apart allow for more accurate risk prediction and may assist in decision-making regarding referral and/or biopsy.18
Prostate biopsy is recommended for men with a total serum PSA of 4.0 ng/mL or greater, regardless of DRE findings. Biopsy at this time increases the likelihood of diagnosing disease while it is still organ-confined.26 In men with serum PSA of 10 ng/mL or more, the chance of finding prostate cancer exceeds 50%, and many such men will have disease that has already extended beyond the prostate.27
Managing men with PSA measurements below 4.0 ng/mL is more difficult. The majority of men in this category will have negative biopsies. However, a significant number of men with prostate cancer present with serum PSA concentrations below 4.0 ng/mL.28 Because cancer detected in these men is likely to be organ-confined, the National Comprehensive Cancer Network altered its guidelines, recommending that prostate biopsy be considered in men with a serum PSA between 2.6 and 4.0 ng/mL; or in those with a rate of rise in the serum PSA (PSA velocity) of at least 0.35 ng/mL/year in men with a serum PSA of 2.5 ng/mL or less.26
DIAGNOSIS
The diagnosis of prostate cancer is accomplished through a histologic examination of biopsied prostate tumor. The biopsy is performed using transrectal ultrasound. A prostate biopsy may be indicated based upon clinical symptoms, an abnormal DRE, or an elevated serum PSA.29
Transrectal ultrasonography with prostate biopsy is indicated in men with DRE findings that are suspicious for cancer (ie, induration, asymmetry, or palpable nodularity of the prostate gland), even if the serum PSA is not elevated; such findings require that prostate cancer be ruled out. This is particularly important if the patient is older than 45 or has other risk factors for the disease.17,30
Tumors located in the posterior and lateral aspects of the prostate gland are most often detected by DRE. About 25% to 35% of prostate tumors develop in other areas of the prostate or are too small to be detected by DRE.31
A serum PSA level should be ordered before biopsy in men with an abnormal DRE for diagnostic and prognostic purposes. Serum PSA concentrations rise slightly during the first several hours after a rectal examination in some men; if possible, the PSA should not be drawn within one week of the DRE but should be obtained prior to the biopsy.18,32
Staging
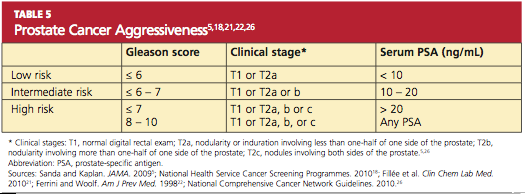
Prostate cancer is divided into low, intermediate, and high risk, based on the serum PSA, the Gleason score, and the clinical stage (see Table 5,5,18,21,22,26 ). Imaging studies, including CT of the abdomen and pelvis, radionuclide bone scans, and endorectal coil MRI, are used selectively to assess for extraprostatic extension, regional adenopathy, or distant metastases.33
PROSTATE BIOPSY
Transrectal biopsy of the prostate is an office procedure. Local and topical anesthetics can be used to minimize associated discomfort,34 although local anesthetics may not completely eliminate the discomfort of the introduction of the probe.35 A combination of local infiltration and topical gel application seems to provide the best pain relief.36 Use of intraprostatic administration of local anesthetic and of NSAID-containing rectal suppositories is currently being explored.37
Many men who undergo prostate biopsy are middle-aged or elderly and may be receiving antiplatelet therapy (most commonly with low-dose aspirin).38 To decrease the risk for bleeding complications, patients should be advised to discontinue antiplatelet therapy seven to 10 days before biopsy, unless even temporary withdrawal places them at increased risk for cardiovascular complications. Continuing antiplatelet drugs does not appear to increase the incidence of severe hemorrhagic complications and is an acceptable option for patients at high risk for cardiovascular incidents.38