Dizziness and Vertigo: Recognizing Vestibular Migraine in the Primary Care Setting





Although accreditation for this CE/CME activity has expired, and the posttest is no longer available, you can still read the full article.
Expires June 30, 2015
–
Vestibular migraine (VM) is the most common cause of recurrent dizziness and vertigo but is often unrecognized by health care providers. VM causes significant impairment in level of function and quality of life, and the diagnosis should be considered when symptoms cannot be explained by other etiologies. Information and guidance are provided to raise clinicians’ awareness of VM in order to increase accurate diagnosis, guide management decisions, and improve patient health outcomes.
TREATMENT OF VM
Nonpharmacologic
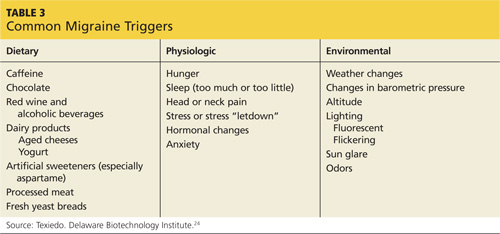
Nonpharmacologic measures to prevent VM attacks include the avoidance of “triggers” through dietary restrictions, stress reduction, and healthy lifestyle modifications. Diaries can be used to help identify common triggers to avoid (see Table 3); patients should understand that it may take up to three months before noticeable improvement in symptoms is seen. Once symptoms have resolved, cautious re-introduction of suspect foods may be attempted.24
Vestibular rehabilitation therapy promotes CNS compensation for inner ear deficits and reduces symptoms of disequilibrium and dizziness.25 It is helpful for complications of VM, such as anxiety, visual dependence, or loss of confidence with balance.10
Pharmacologic
Prophylactic drug therapy is the mainstay of medical management for VM when nonpharmacologic measures are inadequate; episodes are frequent and severe; or symptoms are of long duration.5 The drugs’ adverse effect profiles, as well as patient comorbidities, should guide the choice of therapy.26
Abortive migraine therapies have not been shown to be effective for symptoms of dizziness17 and may cause rebound symptoms. Vestibular suppressants (promethazine, dimenhydrinate, and meclizine) can be used for acute episodes of VM.5
According to evidence-based guidelines for the preventive treatment of migraine in adults,26 the pharmacologic options include multiple drug classes stratified by level, depending on the quality of evidence supporting their effectiveness in migraine prevention.
Level A comprises medications with established efficacy. These include divalproex sodium, sodium valproate, topiramate, frovatriptan (for menstrual migraine), metoprolol, propanolol, and timolol.
Level B medications that are “probably effective” include naratriptan, zolmitriptan, amitriptyline, venlafaxine, atenolol, and nadolol.
Medications that are “possibly effective” are in the Level C category and include carbamazepine, nebivolol, pindolol, lisinopril, candesartan, clonidine, guanfacine, and cyproheptadine.
The Level U category drugs are labeled “inadequate or conflicting data to support or refute medication use” and include fluvoxamine, fluoxetine, protriptyline, gabapentin, bisoprolol, cyclandelate, acenocoumarol, warfarin, picotamide, acetazolamide, nicardipine, nifedipine, nimodipine, and verapamil.
Medications that are established as possibly or probably ineffective fall under the category of Other and include clomipramine, lamotrigine, acebutolol, clonazepam, nabumetone, oxcarbazepine, and telmisartan.
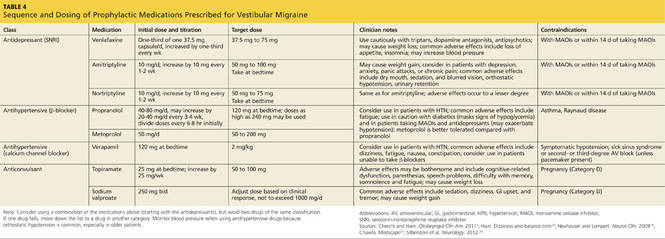
When initiating therapy, low doses are recommended because migraineurs’ sensory hypersensitivity is thought to extend to medications.5 Sequence and dosing information, along with contraindications, should be considered when choosing medical therapies (see Table 4).5,12,19,21,26 Patient response to treatment is evaluated after one to three months, and medications should be discontinued if symptoms persist, maximum dose is reached, or significant adverse effects occur.5 A reasonable goal of therapy is to reduce episode frequency by more than 50%.19 Should both lifestyle modifications and medications fail, referral to a specialist for reevaluation of the diagnosis is warranted.8
On the next page: Conclusion >>