Dizziness and Vertigo: Recognizing Vestibular Migraine in the Primary Care Setting





Although accreditation for this CE/CME activity has expired, and the posttest is no longer available, you can still read the full article.
Expires June 30, 2015
–
Vestibular migraine (VM) is the most common cause of recurrent dizziness and vertigo but is often unrecognized by health care providers. VM causes significant impairment in level of function and quality of life, and the diagnosis should be considered when symptoms cannot be explained by other etiologies. Information and guidance are provided to raise clinicians’ awareness of VM in order to increase accurate diagnosis, guide management decisions, and improve patient health outcomes.
CLINICAL MANIFESTATIONS OF VM
The clinical presentation of VM varies for each patient, as do the frequency and duration of episodes. Manifestations of VM may include5,19,20
• Vertigo associated with visual triggers
• Nausea and/or dizziness
• Spontaneous positional vertigo
• Head motion intolerance
• Motion sickness
• Lightheadedness
• Headache
• Chronic disequilibrium
• Inability to concentrate
• Mild hearing loss or tinnitus
• Cervicalgia
• Anxiety
• Panic
• Photophobia
• Phonophobia
• Sensory aura
Visual vertigo, described as vertigo worsened by visual stimulation such as moving scenes, scrolling patterns, and movement of large crowds or traffic, is highly suggestive of VM.19 Aura-type symptoms are of significant diagnostic importance because they may be the only apparent connection between vertigo and migraine.19
The duration of vertigo and dizziness may range from seconds to weeks. These episodes may have no temporal relationship with headaches. Vertigo and dizziness can continue for more than 24 hours for about half of VM patients; in some, symptoms persist for several weeks or more.12 In addition, vertigo and headache may never occur together, which further increases the diagnostic challenge for this disorder.1,5
Although many hypotheses exist, the pathophysiology of VM remains unclear.
Patient History
It is vital to obtain a detailed medical and social history in order to determine possible etiologies for symptoms. Medications in particular must be reviewed with care because many are known to induce vestibular-type symptoms.
Cardiac agents of potential concern for causing dizziness include β-blockers, diuretics, ACE inhibitors, β-blockers, and nitrates. CNS agents associated with dizziness include antipsychotics, dopaminergic drugs, opioids/analgesics, hypnotics, anticonvulsants, tricyclic antidepressants, and muscle relaxants. Anticholinergics, phosphodiesterase type 5 inhibitors, antibacterials, aminoglycosides, fluoroquinolones, and antineoplastics may also lead to dizziness; several of these medications are also known to be ototoxic. Dizziness can also be related to orthostatic hypotension, which is a common adverse effect of many of the listed medications, especially when used in combination.7,9
Diabetes, hypertension, vascular diseases, and neurologic disorders should be considered as causes for vision and proprioception problems.7 Patients may present with a personal history of headaches for years before vestibular symptoms develop.6 Motion sickness is suggestive of a possible migraine diagnosis.19
Positive family history is common for migraineurs.21 Patients ages 30 to 39 are affected most frequently, with an estimated prevalence of 7% in men and 24.4% in women.22
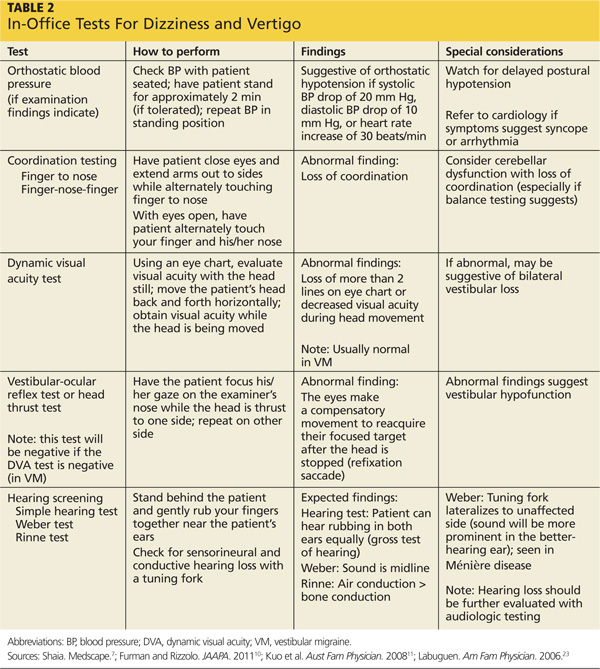
Physical Examination
The focused physical should include cranial nerve assessments, an otoscopic examination, hearing evaluation with a tuning fork, and audiometry, if a hearing deficit is detected. Minor oculomotor abnormalities, such as “weak” nystagmus with vertical, horizontal, torsional, or positional components, may be noted in approximately 70% of patients with VM.5 Various in-office tests (see Table 2) should also be conducted to narrow the possible causes for vertigo and dizziness and rule out more serious disorders.7,10 ,11,23
Diagnostic Workup
Laboratory tests are generally not recommended because they identify the cause of vertigo in only approximately 1% of patients.23 Similarly, routine use of MRI or CT is not recommended, but these modalities may be indicated for patients with focal neurologic deficits or risk factors for cerebrovascular disease, or if acute treatments for peripheral vertigo are unsuccessful.10
On the next page: Treatment >>