Nonallergic rhinitis: Common problem, chronic symptoms





ABSTRACTNonallergic rhinitis can significantly affect a patient’s quality of life. It is difficult to distinguish from allergic rhinitis, but it has different triggers, and its response to treatment can vary. We review its differential diagnosis, causes, and treatment.
KEY POINTS
- When evaluating a patient with rhinitis, a key question is whether it is allergic or nonallergic.
- Identifying triggers that should be avoided is important for controlling symptoms.
- If symptoms continue, then the first-line treatment for nonallergic rhinitis is intranasal steroids.
- Failure of intranasal steroids to control symptoms should prompt a consideration of the many potential causes of rhinitis, and further evaluation and treatment can be tailored accordingly.
Many drugs available
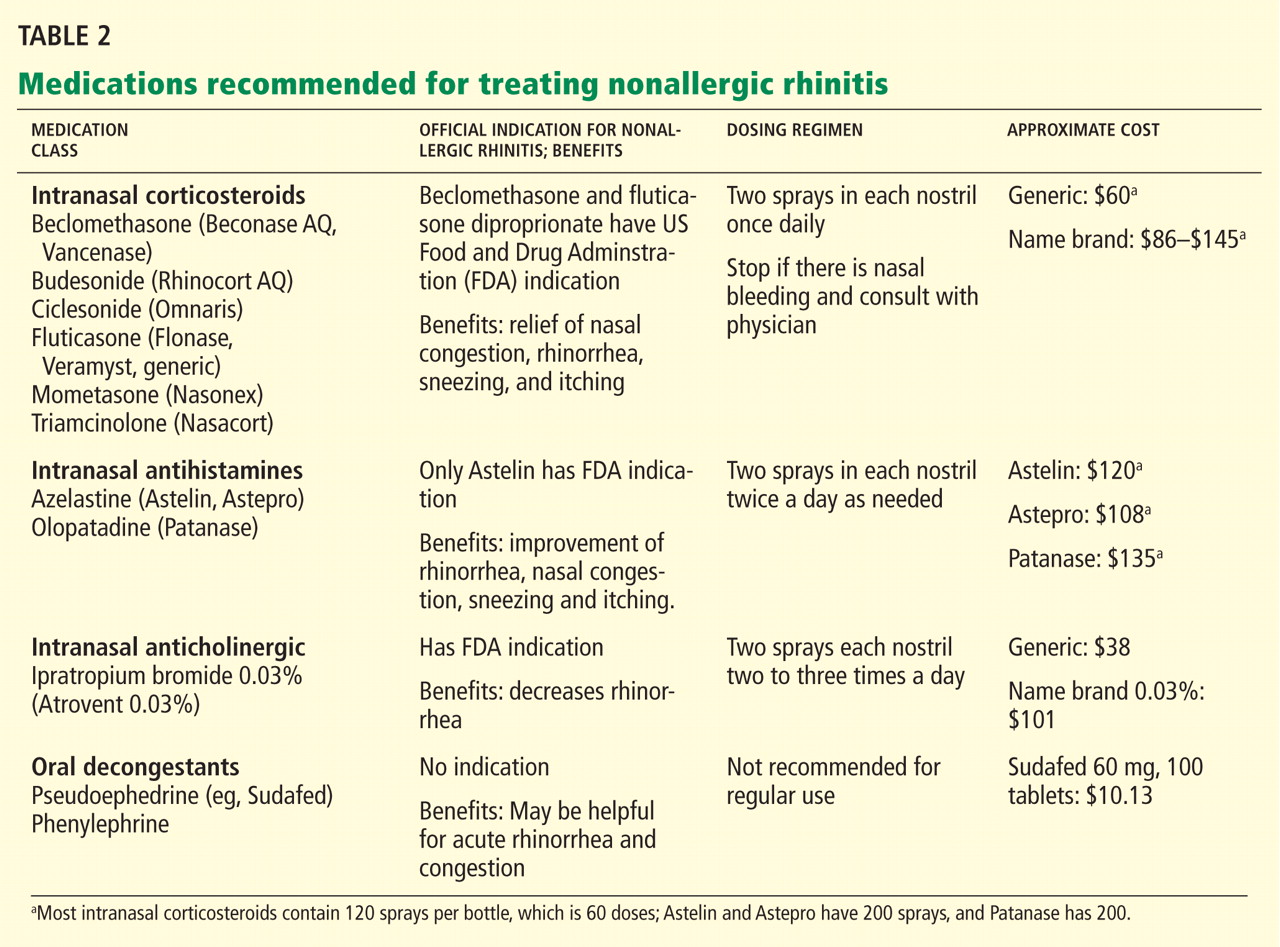
Fortunately, many effective drugs are available to treat nonallergic rhinitis. These have few adverse effects or drug interactions.
Intranasal steroid sprays are considered first-line therapy, as there are studies demonstrating effectiveness in nonallergic rhinitis.22 Intranasal fluticasone propionate (Flonase) and beclomethasone dipropionate (Beconase AQ) are approved by the US Food and Drug Administration (FDA) for treating nonallergic rhinitis. Intranasal mometasone (Nasonex) is approved for treating nasal polyps.
Nasal steroid sprays are most effective if the dominant nasal symptom is congestion, but they have also shown benefit for rhinorrhea, sneezing, and itching.
Side effects of nasal steroid sprays include nasal irritation (dryness, burning, and stinging) and epistaxis, the latter occurring in 5% to 10% of patients.23
Intranasal antihistamines include azelastine (Astelin, Astepro) and olopatadine (Patanase). They are particularly useful for treating sneezing, congestion, and rhinorrhea.24 Astelin is the only intranasal antihistamine with FDA approval for nonallergic rhinitis.
Side effects of this drug class include bitter taste (with Astelin), sweet taste (with Astepro), headache, and somnolence.
Oral antihistamines such as loratadine (Claritin), cetirizine (Zyrtec), and fexofenadine (Allegra) are now available over the counter, and many patients try them before seeking medical care. These drugs may be helpful for those bothered by sneezing. However, no study has demonstrated their effectiveness for nonallergic rhinitis.25 First-generation antihistamines may help with rhinorrhea via their anticholinergic effects.
Ipratropium, an antimuscarinic agent, decreases secretions by inhibiting the nasal parasympathetic mucous glands. Intranasal ipratropium 0.03% (Atrovent 0.03%) should be considered first-line if the dominant symptom is rhinorrhea. Higher-dose ipratropium 0.06% is approved for rhinorrhea related to the common cold or allergic rhinitis. Because it is used topically, little is absorbed. Its major side effect is nasal dryness.
Decongestants, either oral or topical, can relieve the symptoms of congestion and rhinorrhea in nonallergic rhinitis. They should only be used short-term, as there is little evidence to support their chronic use.
Phenylpropanolamine, a decongestant previously found in over-the-counter cough medicines, was withdrawn from the market in 2000 owing to concern that the drug, especially when used for weight suppression, was linked to hemorrhagic stroke in young women.26,27 Other oral decongestants, ie, pseudoephedrine and phenylephrine, are still available, but there are no definitive guidelines for their use. Their side effects include tachycardia, increase in blood pressure, and insomnia.
Nasal saline irrigation has been used for centuries to treat rhinitis and sinusitis, despite limited evidence of benefit. A Cochrane review concluded that saline irrigation was well tolerated, had minor side effects, and could provide some relief of rhinosinusitis symptoms either as the sole therapeutic measure or as adjunctive treatment.28 Hypertonic saline solutions, while possibly more effective than isotonic saline in improving mucociliary clearance, are not as well tolerated since they can cause nasal burning and irritation. Presumed benefits of saline irrigation are clearance of nasal secretions, improvement of nasociliary function, and removal of irritants and pollen from the nose.
A strategy
Imaging the sinuses with CT, which has replaced standard nasal radiography, may help if one is concerned about chronic rhinosinusitis, nasal polyps, or other anatomic condition that could contribute to persistent symptoms. Cost and radiation exposure should enter into the decision to obtain this study because a diagnosis based on the patient’s report of symptoms may be equally accurate.29,30
CASE CONTINUED
Our patient has a number of potential causes of her symptoms. Exposure to second-hand tobacco smoke at home and to the air in airplanes could be acute triggers. Weather and temperature changes could explain her chronic symptoms in the spring and fall. Use of an angiotensin-converting enzyme inhibitor (in her case, lisinopril) and estrogen replacement therapy may contribute to perennial symptoms, but the onset of her nonallergic rhinitis does not correlate with the use of these drugs. There are no symptoms to suggest chronic rhinosinusitis or anatomic causes of her symptoms.
This case is typical of vasomotor rhinitis of the weather- or temperature-sensitive type. This diagnosis may explain her lack of improvement with intranasal steroids, though adherence and spray technique should be assessed. At this point, we would recommend trying topical antihistamines daily when chronic symptoms are present or as needed for acute symptoms.