Nonallergic rhinitis: Common problem, chronic symptoms





ABSTRACTNonallergic rhinitis can significantly affect a patient’s quality of life. It is difficult to distinguish from allergic rhinitis, but it has different triggers, and its response to treatment can vary. We review its differential diagnosis, causes, and treatment.
KEY POINTS
- When evaluating a patient with rhinitis, a key question is whether it is allergic or nonallergic.
- Identifying triggers that should be avoided is important for controlling symptoms.
- If symptoms continue, then the first-line treatment for nonallergic rhinitis is intranasal steroids.
- Failure of intranasal steroids to control symptoms should prompt a consideration of the many potential causes of rhinitis, and further evaluation and treatment can be tailored accordingly.
CLUES POINTING TO NONALLERGIC VS ALLERGIC RHINITIS
Nonallergic rhinitis encompasses a range of syndromes with overlapping symptoms. While tools such as the Rhinitis Diagnostic Worksheet are available to help differentiate allergic from nonallergic rhinitis, debate continues about whether it is necessary to characterize different forms of rhinitis before initiating treatment.8
The diagnosis of nonallergic rhinitis depends on a thorough history and physical examination. Key questions relate to the triggers that bring on the rhinitis, which will assist the clinician in determining which subtype of rhinitis a patient may be experiencing and therefore how to manage it. Clues:
- Patients with nonallergic rhinitis more often report nasal congestion and rhinorrhea, rather than sneezing and itching, which are predominant symptoms of allergic rhinitis.
- Patients with nonallergic rhinitis tend to develop symptoms at a later age.
- Common triggers of nonallergic rhinitis are changes in weather and temperature, food, perfumes, odors, smoke, and fumes. Animal exposure does not lead to symptoms.
- Patients with nonallergic rhinitis have few complaints of concomitant symptoms of allergic conjunctivitis (itching, watering, redness, and swelling).
- Many patients with nonallergic rhinitis find that antihistamines have no benefit. Also, they do not have other atopic diseases such as eczema or food allergies and have no family history of atopy.
PHYSICAL FINDINGS
Some findings on physical examination may help distinguish allergic from nonallergic rhinitis.
- Patients with long-standing allergic rhinitis may have an “allergic crease,” ie, a horizontal wrinkle near the tip of the nose caused by frequent upward wiping. Another sign may be a gothic arch, which is a narrowing of the hard palate occurring as a child.
- In allergic rhinitis, the turbinates are often pale, moist, and boggy with a bluish tinge.

CASE CONTINUED
Our patient’s symptoms can be caused by many different factors. Allergic triggers for rhinitis include both indoor and outdoor sources. The most common allergens include cat, dog, dust mite, cockroach, mold, and pollen allergens. The absence of acute sneezing and itching when around her cat and her recent negative skin-prick tests confirm that the rhinitis symptoms are not allergic.
In this patient, who has symptoms throughout the year but no allergic triggers, consideration of the different subtypes of nonallergic rhinitis may help guide further therapy.
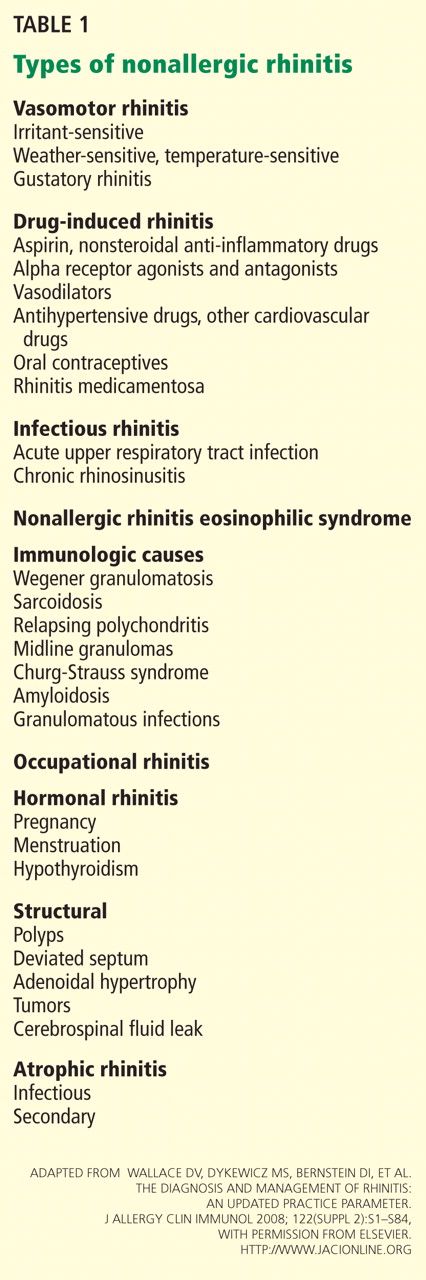
SUBTYPES OF NONALLERGIC RHINITIS
Vasomotor rhinitis
Vasomotor rhinitis is thought to be caused by a variety of neural and vascular triggers, often without an inflammatory cause. These triggers lead to symptoms involving nasal congestion and clear rhinorrhea more than sneezing and itching. The symptoms can be sporadic, with acute onset in relation to identifiable nonallergic triggers, or chronic, with no clear trigger.
Gustatory rhinitis, for example, is a form of vasomotor rhinitis in which clear rhinorrhea occurs suddenly while eating or while drinking alcohol. It may be prevented by using nasal ipratropium (Atrovent) before meals.
Irritant-sensitive vasomotor rhinitis. In some patients, acute vasomotor rhinitis symptoms are brought on by strong odors, cigarette smoke, air pollution, or perfume. When asked, most patients easily identify which of these irritant triggers cause symptoms.
Weather- or temperature-sensitive vasomotor rhinitis. In other patients, a change in temperature, humidity, or barometric pressure or exposure to cold or dry air can cause nasal symptoms.9 These triggers are often hard to identify. Weather- or temperature-sensitive vasomotor rhinitis is often mistaken for seasonal allergic rhinitis because weather changes occur in close relation to the peak allergy seasons in the spring and fall. However, this subtype does not respond as well to intranasal steroids.9
Other nonallergic triggers of vasomotor rhinitis may include exercise, emotion, and sexual arousal (honeymoon rhinitis).10
Some triggers, such as tobacco smoke and perfume, are easy to avoid. Other triggers, such as weather changes, are unavoidable. If avoidance measures fail or are inadequate, medications (described below) can be used for prophylaxis and symptomatic treatment.
Drug-induced rhinitis
Drugs of various classes are known to cause either acute or chronic rhinitis. Drug-induced rhinitis has been divided into different types based on the mechanism involved.11
The local inflammatory type occurs in aspirin-exacerbated respiratory disease, which is characterized by nasal polyposis with chronic rhinosinusitis, hyposmia, and moderate to severe persistent asthma. Aspirin and other NSAIDs induce an acute local inflammation, leading to severe rhinitis and asthma symptoms. Avoiding all NSAID products is recommended; aspirin desensitization may lead to improvement in rhinosinusitis and asthma control.
The neurogenic type of drug-induced rhinitis can occur with sympatholytic drugs such as alpha receptor agonists (eg, clonidine [Cat-apres]) and antagonists (eg, prazosin [Minipress]).11 Vasodilators, including phosphodiesterase-5 inhibitors such as sildenafil (Viagra), can lead to acute rhinitis symptoms (“anniversary rhinitis”).
Unknown mechanisms. Many other medications can lead to rhinitis by unknown mechanisms, usually with normal findings on physical examination. These include beta-blockers, angiotensin-converting enzyme inhibitors, calcium channel blockers, exogenous estrogens, oral contraceptives, antipsychotics, and gabapentin (Neurontin).
Correlating the initiation of a drug with the onset of rhinitis can help identify offending medications. Stopping the suspected medication, if feasible, is the first-line treatment.
Rhinitis medicamentosa, typically caused by overuse of over-the-counter topical nasal decongestants, is also classified under drug-induced rhinitis. Patients may not think of nasal decongestants as medications, and the physician may need to ask specifically about their use.
On examination, the nasal mucosa appears beefy red without mucous. Once a diagnosis is made, the physician should identify and treat the original etiology of the nasal congestion that led the patient to self-treat.
Patients with rhinitis medicamentosa often have difficulty discontinuing use of topical decongestants. They should be educated that the withdrawal symptoms can be severe and that more than one attempt at quitting may be needed. To break the cycle of rebound congestion, topical intranasal steroids should be used, though 5 to 7 days of oral steroids may be necessary.1
Cocaine is a potent vasoconstrictor. Its illicit use should be suspected, especially if the patient presents with symptoms of chronic irritation such as frequent nosebleeds, crusting, and scabbing.12
Infectious rhinitis
One of the most common causes of acute rhinitis is upper respiratory infection.
Acute viral upper respiratory infection often presents with thick nasal discharge, sneezing, and nasal obstruction that usually clears in 7 to 10 days but can last up to 3 weeks. Acute bacterial sinusitis can follow, typically in fewer than 2% of patients, with symptoms of persistent nasal congestion, discolored mucus, facial pain, cough, and sometimes fever.
Chronic rhinosinusitis is a syndrome with sinus mucosal inflammation with multiple causes. It is clinically defined as persistent nasal and sinus symptoms lasting longer than 12 weeks and confirmed with computed tomography (CT).13 The CT findings of chronic rhinosinusitis include thickening of the lining of the sinus cavities or complete opacification of the pneumatized sinuses.
Major symptoms to consider for diagnosis include facial pain, congestion, obstruction, purulent discharge on examination, and changes in olfaction. Minor symptoms are cough, fatigue, headache, halitosis, fever, ear symptoms, and dental pain.
Treatment may involve 3 or more weeks of an oral antibiotic and a short course of an oral steroid, a daily nasal steroid spray, or both oral and nasal steroids. Most patients can be managed in the primary care setting, but they can be referred to an ear, nose, and throat specialist, an allergist, or an immunologist if their symptoms do not respond to initial therapy.