Nonallergic rhinitis: Common problem, chronic symptoms





ABSTRACTNonallergic rhinitis can significantly affect a patient’s quality of life. It is difficult to distinguish from allergic rhinitis, but it has different triggers, and its response to treatment can vary. We review its differential diagnosis, causes, and treatment.
KEY POINTS
- When evaluating a patient with rhinitis, a key question is whether it is allergic or nonallergic.
- Identifying triggers that should be avoided is important for controlling symptoms.
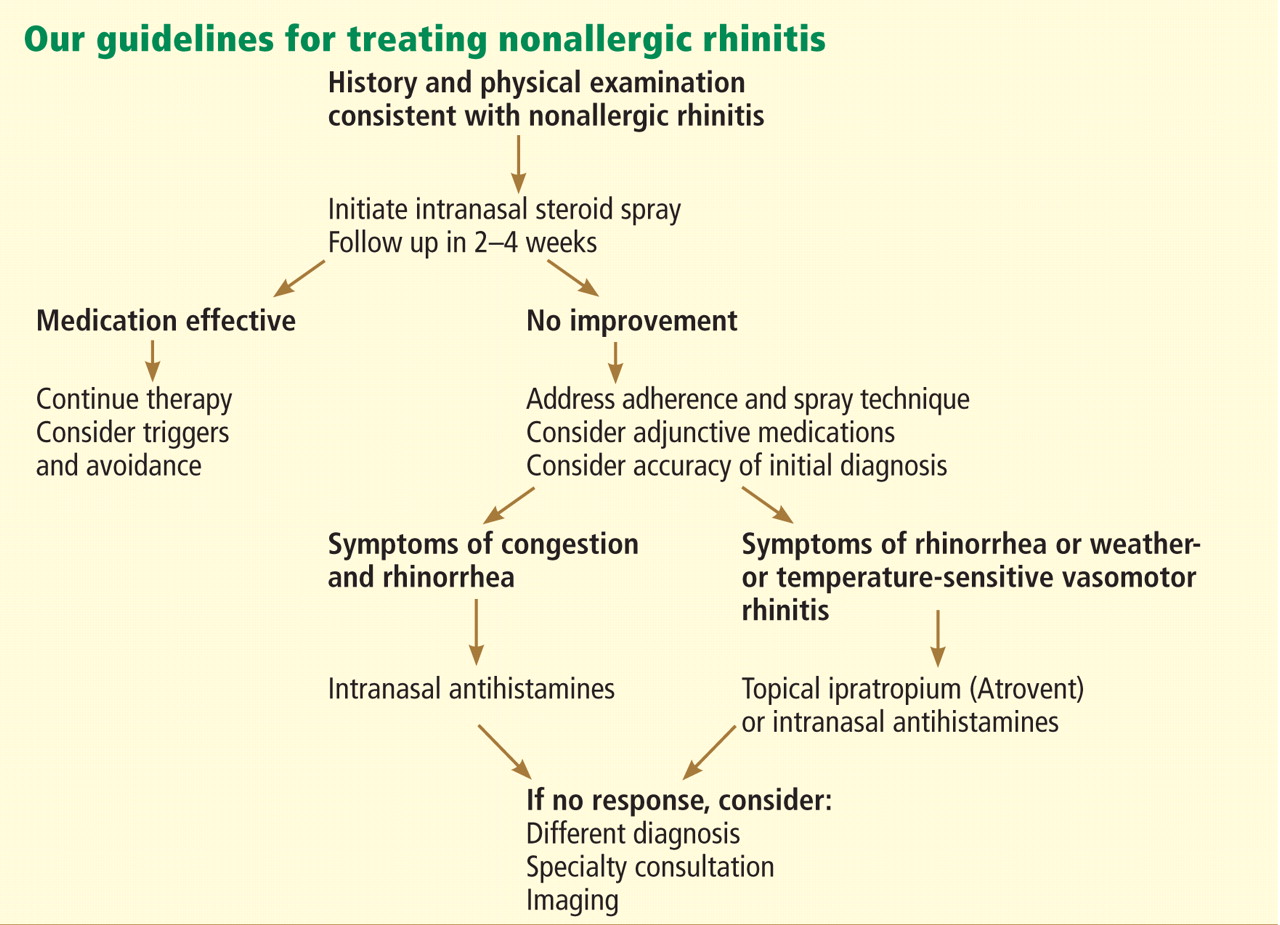
- If symptoms continue, then the first-line treatment for nonallergic rhinitis is intranasal steroids.
- Failure of intranasal steroids to control symptoms should prompt a consideration of the many potential causes of rhinitis, and further evaluation and treatment can be tailored accordingly.
Nonallergic rhinitis eosinophilic syndrome
Patients with nonallergic rhinitis eosinophilic syndrome (NARES) are typically middle-aged and have perennial symptoms of sneezing, itching, and rhinorrhea with intermittent exacerbations. They occasionally have associated hyposmia (impaired sense of smell).1 The diagnosis is made when eosinophils account for more than 5% of cells on a nasal smear and allergy testing is negative.
Patients may develop nasal polyposis and aspirin sensitivity.1 Entopy has been described in some.14
Because of the eosinophilic inflammation, this form of nonallergic rhinitis responds well to intranasal steroids.
Immunologic causes
Systemic diseases can affect the nose and cause variable nasal symptoms that can be mistaken for rhinitis. Wegener granulomatosis, sarcoidosis, relapsing polychondritis, midline granulomas, Churg-Strauss syndrome, and amyloidosis can all affect the structures in the nose even before manifesting systemic symptoms. Granulomatous infections in the nose may lead to crusting, bleeding, and nasal obstruction.1
A lack of a response to intranasal steroids or oral antibiotics should lead to consideration of these conditions, and treatment should be tailored to the specific disease.
Occupational rhinitis
Occupational exposure to chemicals, biologic aerosols, flour, and latex can lead to rhinitis, typically through an inflammatory mechanism. Many patients present with associated occupational asthma. The symptoms improve when the patient is away from work and worsen throughout the work week.
Avoiding the triggering agent is necessary to treat these symptoms.
Hormonal rhinitis
Hormonal rhinitis, ie, rhinitis related to metabolic and endocrine conditions, is most commonly associated with high estrogen states. Nasal congestion has been reported with pregnancy, menses, menarche, and the use of oral contraceptives.15 The mechanism for congestion in these conditions still needs clarification.
When considering drug therapy, only intranasal budesonide (Rhinocort) has a pregnancy category B rating.
While hypothyroidism and acromegaly have been mentioned in reviews of nonallergic rhinitis, evidence that these disorders cause nonallergic rhinitis is not strong.16,17
Structurally related rhinitis
Anatomic abnormalities that can cause persistent nasal congestion include nasal septal deviation, turbinate hypertrophy, enlarged adenoids, tumors, and foreign bodies. These can be visualized by simple anterior nasal examination, nasal endoscopy, or radiologic studies. If structural causes lead to impaired quality of life or chronic rhinosinusitis, then consider referral to a specialist for possible surgical treatment.
Clear spontaneous rhinorrhea, with or without trauma, can be caused by cerebrospinal fluid leaking into the nasal cavity.18 A salty, metallic taste in the mouth can be a clue that the fluid is cerebrospinal fluid. A definitive diagnosis of cerebrospinal fluid leak is made by finding beta-2-transferrin in nasal secretions.
Atrophic rhinitis
Atrophic rhinitis is categorized as primary or secondary.
Primary (idiopathic) atrophic rhinitis is characterized by atrophy of the nasal mucosa and mucosal colonization with Klebsiella ozaenae associated with a foul-smelling nasal discharge.19,20 This disorder has been primarily reported in young people who present with nasal obstruction, dryness, crusting, and epistaxis. They are from areas with warm climates, such as the Middle East, Southeast Asia, India, Africa, and the Mediterranean.
Secondary atrophic rhinitis can be a complication of nasal or sinus surgery, trauma, granulomatous disease, or exposure to radiation.21 This disorder is typically diagnosed with nasal endoscopy and treated with daily saline rinses with or without topical antibiotics.21
CASE CONTINUED
Questioned further, our patient says her symptoms are worse when her husband smokes, but that she continues to have congestion and rhinorrhea when he is away on business trips. She notes that her symptoms are often worse on airplanes (dry air with an acute change in barometric pressure), with weather changes, and in cold, dry environments. Symptoms are not induced by eating.
We note that she started taking lisinopril 2 years ago and conjugated equine estrogens 8 years ago. Review of systems reveals no history of facial or head trauma, polyps, or hyposmia.
The rhinitis and congestion are bilateral, and she denies headaches, acid reflux, and conjunctivitis. She has a mild throat-clearing cough that she attributes to postnasal drip.
On physical examination, her blood pressure is 118/76 mm Hg and her pulse is 64. Her turbinates are congested with clear rhinorrhea. The rest of the examination is normal.
AVOID TRIGGERS, PRETREAT BEFORE EXPOSURE
People with known environmental, non-immunologic, and irritant triggers should be reminded to avoid these exposures if possible.
If triggers are unavoidable, patients can pretreat themselves with topical nasal sprays before exposure. For example, if symptoms occur while on airplanes, then intranasal steroids or antihistamine sprays should be used before getting on the plane.