Fetal pulse oximetry: 8 vital questions






Will this noninvasive technique improve assessment of fetal well-being? The authors analyze what the evidence to date does and does not tell.
Other trials underway. The ongoing Fetal Oximetry (FOX) trial of the National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network, involving 10,000 nulliparous participants, is comparing cesarean delivery rates and safety outcomes in patients monitored for FHR plus pulse oximetry with a group in which the clinicians are blinded to the pulse oximetry readings. Another randomized controlled trial of fetal pulse oximetry is underway in Australia.
Potential for increased costs. The American College of Obstetricians and Gynecologists (ACOG) has raised concerns about the potential increase in costs without demonstrable improvement in outcome.5 ACOG has not endorsed fetal pulse oximetry for general practice.
Question 1How accurately does pulse oximetry reflect the fetal condition?
It yields only indirect information on the partial pressure of oxygen in the blood and no data on perfusion or acid-base status.
In other clinical settings, oxygen saturation is not an acceptable substitute for arterial blood gas analysis. The pulse oximeter is not a hemoximeter—only that device directly and reliably determines blood oxygen saturation by spectrophotometry.6 Even the calculated oxygen saturation values provided automatically by modern blood gas analyzers are inaccurate.7
Studies report varying results. In a comparison8 of fetal oxygen saturation by hemoximetry in a fetal scalp blood (FSB) sample and fetal arterial oxyhemoglobin saturation (FSpO2) by pulse oximetry immediately before the blood sampling, the FSpO2 medians were always higher than the FSB hemoximetry saturation—which led to false-negative results in hypoxic babies.
In animal studies, pulse oximetry correlated well with simultaneously measured arterial oxygen saturation (r = 0.98, P = .01),9 but data from human studies are inconsistent. While McNamara et al10 reported good correlation between FSpO2 measurements and umbilical artery blood oxygen saturation at birth (r = 0.59, P <.001), Langer et al11 found no relationship between FSpO2 levels determined during pushing efforts and oxygen saturation in umbilical vein blood at birth.
Possible reasons for the ambiguous findings:
- differences in practice, such as use of umbilical venous versus arterial blood, or measurement during pushing versus between pushes,
- different intervals from FSpO2 reading to umbilical blood sampling, or
- incomparable groups, such as all women in labor versus those with abnormal FHR.
Limitations. Fetal pulse oximetry measures arterial oxygen saturation during the systolic pulse wave in the skin microcirculation at head level. In the fetus, this is part of the preductal circulation, with oxygen saturation levels somewhere between umbilical arterial and umbilical venous blood oxygen saturation.
Theoretically, FSpO2 should be closer to FSB than to umbilical blood. Although FSB samples consist of capillary blood, which is not exactly central arterial blood, the differences are small, at least in the neonate.12 In the intrapartum period, however, several variables with unknown effect may weaken relationships:
- different intervals between the last oximetry signal and blood sampling after delivery
- differences in local tissue perfusion status13
- perfusion changes during fetal compromise, as the fetus centralizes its blood flow, with vasoconstriction in the skin circulation
Question 2What is the critical threshold for fetal oxygen desaturation?
Human studies indicate that an FSpO2 of 33% is approximately the 10th percentile on the normal distribution, and an FSpO2 of 29% to 30% represents the third to fifth percentiles in normal-outcome labor.14 Studies in catheterized fetal sheep suggest that the level below which metabolic acidosis can be anticipated is an FSpO2 of about 30%.15
The 30% threshold also is supported by prospective human data from a multicenter trial.16 According to those data, an FSpO2 of less than 30% has 100% sensitivity in predicting an FSB pH below 7.20. FSpO2 of less than 30% also correlated with a lack of variability on the FHR tracing.17
The cutoff of 30% should not be interpreted as an indication of fetal distress, however. Rather, it represents a threshold below which increasing fetal acidosis will be encountered ( FIGURE 1). Oxygen saturation is a dynamic biologic parameter with broad variation.
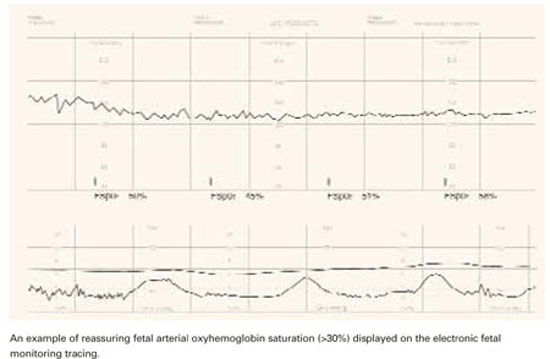
FIGURE 1 Tracking fetal arterial oxyhemoglobin saturation
Question 3Is a single reading reliable?
The normal fetus has a remarkable capacity to compensate for transient episodes of desaturation. Thus, a single reading cannot reflect the fetal condition; the trend in FSpO2 must be taken into account. Research indicates only FSpO2 levels below 30% for more than 2 minutes18 or more than 10 minutes19 are likely to be associated with intrapartum acidosis.
ACOG has raised concerns about the potential increase in costs without demonstrable improvement in outcome.
Gorenberg et al20 retrospectively correlated FSpO2 with umbilical artery pH and found that neither the 30% threshold alone nor the duration of FSpO2 below 30% correlated with fetal acidemia (pH below 7.20). Rather, the repetition of such episodes was more predictive. The authors concluded that more than 10 episodes of FSpO2below 30% would overcome the ability of the fetus to compensate.