Chronic pelvic pain: 11 critical questions about causes and care





An expert explores anatomic and mechanistic bases of chronic pelvic pain in women to clarify optimal diagnosis, management, and treatment
IN THIS ARTICLE
2. How many women suffer chronic pelvic pain?
Chronic pelvic pain is more common than is generally recognized. Here are some estimates:
- A US study conducted by the Gallup organization found that 15% of women 18 to 50 years old had CPP3
- A survey of women in family medicine and ObGyn offices found that 39% had CPP, although only 8% reported having it more often than “sometimes”4
- The Oxfordshire Women’s Health Study, a postal questionnaire survey of a random sample of women 18 to 49 years old in the general UK population, found a prevalence of 24%5
- A primary-care database in a UK study of women 15 to 73 years old found a prevalence of 38 cases for every 1,000 women. (The database contained annualized data that excluded women who had only dysmenorrhea or dyspareunia.) Although the study likely underestimated the prevalence of CPP, the finding does make it possible to compare prevalences in the same population: asthma (37/1,000), back pain (41/1,000), and migraine (21/1,000).6
3. What are the main types of pain involved?
They are nociceptive, inflammatory, and neuropathic pain.
Nociceptive pain occurs in response to a noxious stimulus that alerts the organism to impending tissue injury. One way to think of nociceptive pain is as “normal” or physiologic pain (FIGURE).
Acute pelvic pain is usually nociceptive in origin. CPP is usually not solely nociceptive in origin. It often involves inflammatory or neuropathic pain, or both (TABLE 1).
Inflammatory pain arises in response to tissue injury and the resulting inflammatory process. In some cases, the inflammatory response is actually a source of tissue injury (e.g., rheumatoid arthritis). Inflammatory pain may be an important mechanism in both acute and chronic pelvic pain.
Neuropathic pain is produced by damage to or dysfunction of neurons in the peripheral or central nervous system. It is not physiologic and is often a significant mechanism in the generation of CPP.
An understanding of inflammatory and neuropathic mechanisms is not esoteric, but has clinical significance.
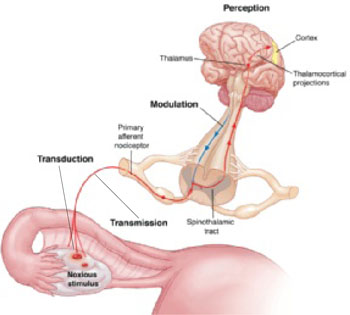
FIGURE Noxious stimulus is often the trigger in acute and chronic pain
Nociceptive pain is a response to a noxious stimulus, alerting the organism to impending tissue injury. Four fundamental processes are involved in nociceptive pain: transduction, in which the stimulus is converted to a biochemical signal; transmission, in which the signal is transported from the peripheral nervous system to the dorsal ganglion and central nervous system; modulation, in which the intensity of the signal is increased or decreased; and perception, in which the organism experiences the pain.TABLE 1
Anatomic and mechanistic classification of pain
Central
|
Peripheral
|
4. Is chronic pelvic pain a disease—or a symptom?
My experience caring for patients who have CPP suggests that chronic pain is a disease, whereas acute pain is a symptom. This concept is controversial in gynecology, and CPP is often labeled as only a symptom, not a diagnosis.7 The search for one underlying disease means that the woman who has CPP frequently undergoes multiple surgical and other invasive procedures, often with incomplete or insignificant diagnoses and responses.
The assumption that CPP is always due to a specific pathologic process in somatic structures or viscera (nociceptive pain) excludes the possibility that CPP can be caused by prolonged or permanent dysfunction of the peripheral or central nervous system, or both (neuropathic pain), or by psychological mechanisms (central pain). Clinical knowledge lags behind basic science in this area and is not at all concrete.
Our ability to accurately diagnose neuropathic or inflammatory pain leaves room for improvement.
5. Is chronic pelvic pain a gynecologic disorder?
Gynecologists have traditionally thought of CPP as either gynecologic or nongynecologic in origin, but this framework has very limited clinical utility. An anatomic and mechanistic classification (TABLE 1) represents a far richer strategic approach to the diagnostic evaluation of CPP, allowing more comprehensive and effective treatment.
6. What distinguishes visceral from somatic pain?
In addition to recognizing the importance of nociceptive, inflammatory, and neuropathic mechanisms in the generation of CPP, it is useful to classify potential causes anatomically (TABLE 1). In the broadest anatomic categories, pain may be central or peripheral, or both. Central pain can be psychogenic or neurogenic, and peripheral pain can be visceral or somatic.
Visceral sources of CPP include the reproductive, genitourinary, and gastrointestinal (GI) tracts. Mechanistically, as has been discussed, visceral pain can be neuropathic, inflammatory, or nociceptive.
Potential somatic sources of CPP are myofascial, skeletal, and cutaneous. Mechanisms leading to somatic CPP can be neuropathic, inflammatory, or nociceptive.
Somatic pain is better understood than visceral pain, but knowledge about the latter has been expanding rapidly. Several characteristics distinguish visceral pain: