Major vascular injury during laparoscopy: Pearls to cope





IN THIS ARTICLE
If the angle of insertion is 45° (≥34°) in the sagittal plane at the umbilicus, puncture safely avoids the aortic bifurcation.
FIGURE 2 At risk: The right common iliac artery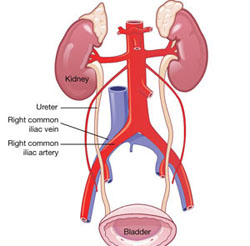
The right common iliac artery overlies its corresponding vein, which puts the artery at risk of injury at initial insertion of the Veress needle.
Tips to facilitate entry
After insufflation, the distance from the base of the navel to the peritoneum is approximately 1.5 to 2.0 cm (FIGURE 3).7 It is neither necessary nor prudent to bury the needle to its hub when placing the initial trocar. Some authors report that over-inflation to 25 mm Hg lowers the risk of vascular injury, creating a longer distance to the retroperitoneal structures.8 In addition, the reduction of tenting means that less force is required.
Patients with a high BMI are likely to be protected from MVI, given the greater distances to major vessels.9 The distance between the entry trocar and retroperitoneal vessels increases directly with BMI, commensurate with increasing abdominal-wall thickness (FIGURE 4).
FIGURE 3 The umbilicus is at its thinnest at low body weight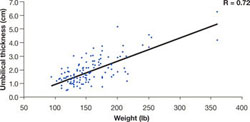
The distance (cm) into the peritoneal cavity after insufflation correlates with a patient’s weight.
SOURCE: Milad and Terkildsen.7
FIGURE 4 How far is it from umbilical skin to the peritoneum and vascular structures?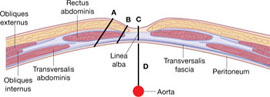
SOURCE: Hurd et al.9
Even optical trocars have been associated with MVI. Between 1994 and 2002, 79 serious complications, including 37 MVIs, were associated with use of these trocars.10
Direct insertion, open technique, and optical trocars have not been studied in comparable numbers. Although the Hasson cannula was not associated with MVI in two large trials involving 10,840 and 5,284 procedures, respectively, there have been case reports to the contrary.11-14
Rubinstein and colleagues15 evaluated the efficacy and safety of the radial dilating trocar VersaStep (US Surgical) for laparoscopic access. This trocar system has a blunt tip and circumferentially dilates rather than directly incising the fascia of the abdominal wall. Use of the blunt-tip trocar may decrease the incidence of initial access injury.
3. Don’t be the King or Queen of denial
Because MVI is estimated to occur in one in every 1,000 to one in every 10,000 procedures, and a typical gynecologic surgeon performs roughly 12 laparoscopies a year, it is unlikely that he or she will encounter more than one MVI over the course of a career. Nevertheless, when a retroperitoneal hematoma or brisk bleeding is visualized at laparoscopy, an MVI should immediately be suspected.
Do not enter into a state of denial and attempt to manage this complication conservatively. The earlier the MVI can be diagnosed, the better the outcome. A retroperitoneal hematoma, dark venous blood pooling in the abdomen, and bright red pulsatile blood are all signs of MVI. Do not wait for systemic changes such as hypotension or cardiac arrhythmias, as these are late findings.
4. No man is an island. Get help when you need it!
As residents, we had the shoulder-dystocia drill burned into memory, the first step being: “Call for help.” Regrettably, there is much less emphasis placed on the need to call for help in a surgical emergency.
All members of the surgical team should be notified of the situation and its associated gravity. The anesthesia team will need to ensure that there are adequate intravenous (IV) access, IV fluids, and blood products for resuscitation. The circulator will need to recruit help so that there will be additional hands to call consults, obtain blood, bring in abdominal trays, scrub in and retract, and so on.
5. Identify, secure, and control the site of injury
Just as a pilot must memorize the early response to an emergency, so must a surgeon be prepared for MVI. In the setting of potential catastrophic hemorrhage, time is of the essence.
The first task is to stay calm and avoid panic. Your role as the surgeon is to identify, secure, and control the site of injury while other team members work on their duties.
Laparoscopy usually not an option 2
It is the rare laparoscopic surgeon who can manage catastrophic hemorrhage endoscopically. It usually is best to remove the trocar from the vessel wall and convert to laparotomy. Attempting to leave a trocar in a vessel may extend the injury and create greater trauma to the vessel.
It is likely that patients will need to undergo secondary procedures if traditional laparoscopic interventions are used.
A vertical skin incision is best
The vertical incision is preferable because it allows greater access and visibility. Sadly, that information does not seem to translate into common practice. One study reported that 27 of 31 women with vascular injury were opened with a Pfannenstiel incision for emergency laparotomy.16