Surgical strategies to untangle a frozen pelvis





Few surgeries require the judgment, rigorous experience, and skill necessary to operate on a frozen pelvis
IN THIS ARTICLE
At one time or another, every surgeon finds it necessary to rethink a planned procedure after the operation begins—a not uncommon scenario during surgery in the frozen pelvis. It can occur at the beginning of a procedure, once the incision is made and the pathology is surveyed, or it can arise when the surgeon is well into an operation, when all the usual landmarks are indistinguishable.
When the problem is clear from the get-go
When confronted with an impossible situation upon opening the abdomen, the surgeon has 2 options:
- close the abdomen and refer the patient
- call for the aid of a surgical colleague who has the necessary experience and skill.
When the operation is under way
This situation may not lend itself to so easy a solution. When the surgeon becomes overwhelmed by an unfamiliar operative field, he or she should stop operating, take stock of what has been accomplished and what remains to be done, check the status of the patient, and reevaluate the case. Again, 2 options are available:
- change the original goal and terminate the procedure at that point, scheduling reoperation for a later date
- call for help, particularly if arrangements have been made beforehand.
Either way, a compromised patient is too high a price to pay for the sake of the surgeon’s vanity, and the dictum of “primum non nocere” should become the guiding principle.
Choose entry into the retroperitoneum with care
Once you have identified the structures, determine how you will be entering the retroperitoneum. This decision is important because the blood supply to the uterus and adnexa lies in the retroperitoneum, as do the ureters, which must be identified and kept under direct vision during ligation of the IP ligaments and dissection of the peritoneum around the uterus.
Retroperitoneal entry and elaboration of the retroperitoneal spaces are keys to the safe performance of a difficult hysterectomy or removal of retained adnexa in a patient with a frozen pelvis. The retroperitoneal approach makes it possible to reach around structures that are fixed in the pelvis, to identify the blood supply and other vital structures, and to proceed safely.
Several entry sites are possible. In the frozen pelvis, I believe the round ligament is the ideal location. Identify and divide this ligament as it enters the internal ring, and incise the peritoneum cephalad along the course of the IP ligaments (FIGURE 2).
FIGURE 2 Transect the round ligaments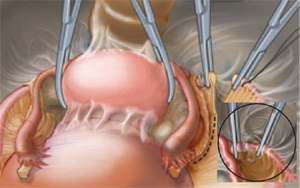
To facilitate entry into the retroperitoneum, transect the round ligaments. Then develop the retroperitoneal spaces using blunt dissection.Next, open the pararectal space to visualize the iliac vessels and ureter, which can be identified on the medial leaf of the peritoneum. The IP ligaments can then be visualized and safely divided. Extending the dissection caudad allows entry into the retrovesical space and into areas of the broad ligament adjacent to the uterus. This approach also makes it possible to produce traction on the peritoneum and facilitate separation of the areolar tissue between the bladder and cervix to enter the vesicovaginal space. Continue dissection of the bladder from the cervix and vagina by operating from one side of the pelvis to the other.
The ureter, a surgeon’s nemesis
Never assume you know the position of the ureter without confirming it; a major deviation of its course can occur secondary to pathologic processes in the pelvis. The ureter can be identified by direct visualization, peristalsis, and palpation. If it is rolled between the thumb and forefinger, the ureter produces a snapping sensation.
After entering the retroperitoneum, identify the ureter between the pelvic brim and Wertheim’s tunnel. Although it may, at times, be seen through the thin peritoneum as it travels over the common iliac artery down into the pelvis, the ureter is generally not clearly visualized in the frozen pelvis and may become apparent only after the peritoneum has been opened and the retroperitoneal spaces elaborated.
Near the level of the pelvic brim on the left side of the body, the ureter will be closer to the IP ligament than it is on the right side, due to the location of the sigmoid colon and its mesentery on the left side, which elevate the ureter in the ventral direction.
Once the ureter has been identified, leave it attached to the peritoneum as much as possible. When the ureter is adherent to pelvic pathology, lateralize it from the medial leaf of the broad ligament as far down into the pelvis as necessary to allow complete removal of the peritoneum along with the pathology. The extent of dissection necessary will vary with the pathology.