Two-Year Experience of 14 French Pigtail Catheters Placed by Procedure-Focused Hospitalists





BACKGROUND: Recent studies show small-bore chest tubes, commonly 14 French pigtail catheters (PCs), are noninferior to large-bore chest tubes for treating various conditions, and they are associated with better patient comfort. The Medical College of Wisconsin implemented a bedside procedure service (BPS) that has been trained in the placement of PCs as an adjunct to its interventional radiology department.
METHODS: The data regarding consults for PC placement was collected by the BPS over a 2-year period. Primary outcomes reviewed were insertion-related complications (IRCs), unsuccessful attempts (UAs), and adverse outcomes (AOs) because the authors believe these represent the safety and effectiveness of the group. It was determined which services consulted the BPS for PC placement, the indications for consults, and a brief review of declined PC consults.
RESULTS: Of the 124 accepted consults, the service had 3 IRCs (2.4%), 2 UAs (1.6%), and 3 AOs (2.4%). A total of 18 consults were declined. The BPS was consulted by 12 services with 8 primary reasons for PC placement.
CONCLUSIONS: At high-volume, tertiary care centers, and with the support of cardiothoracic surgical and interventional radiology services, procedure-focused hospitalists can safely serve as an adjunct service for PC placement in selected hospitalized patients.
© 2020 Society of Hospital Medicine
RESULTS
Over a 2-year period, the BPS was consulted to place 142 PCs. After resolution of the 3 discrepancies, total consults remained 142, PC attempts totaled 124 (87.3%), and declined consults totaled 18 (12.7%).
The 18 declined consults were not performed for reasons relating to procedural safety. These included 15 (83.3%) for insufficient fluid depth, 1 (5.6%) poor window for PTX, and 1 (5.6%) patient unstable per BPS attending judgement. One (5.6%) final consult had a previous drain in same hemithorax that resumed functioning.
The manual chart review of procedures performed 48 hours after declined PC consults found only 3 of 17 (17.6%) patients received a PC within the subsequent 48 hours. The 18th patient was unable to be followed in our electronic medical record because his medical record number was recorded incorrectly.
The remaining 124 consults were deemed safe for PC placement. Indications for PC placement varied; the most common indications were complicated effusion (36.3%), large or recurrent effusions (21.8%), PTX (17%), and hemothorax (HTX; 17%). The most common teams who consulted the BPS for PC were medicine/hospitalists (42.7%) and CT surgery (40.3%).
Three UAs were charted in the database, but on review it was determined that only 2 (1.6%) qualified as UAs (Table 3). A PC was attempted with the UA patient No. 3 for a loculated apical PTX. It is clear in the procedure note that the pleural space was accessed, air was appropriately drained, and a PC was advanced safely into the pleural space; however, the PC then stopped draining air. CXR interpretation also noted “pneumothorax described on prior exam is less evident.” Because the pleural space was accessed safely and had a partially therapeutic response, we do not count this PC placement as a UA. The PC may count as “failed,” but determination of a “failure rate” is not the intent of this paper. This point is further discussed in the Discussion section.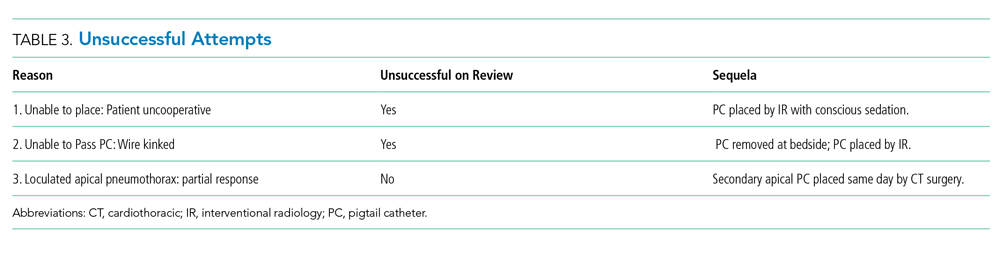
In addition, chart review demonstrated that UA patient No. 3 required intubation within the 24-hour period after our PC attempt, which is an AO. Approximately 10 hours after our PC was placed and removed, CT surgery placed a second PC, and 3 hours after their PC placement, the patient was intubated with subsequent bronchoscopy. The patient was extubated after only 17 hours. This sequence of events suggests mucus plugging as a more likely cause for respiratory failure than our PC attempt, but we have included it as an AO given the time frame.
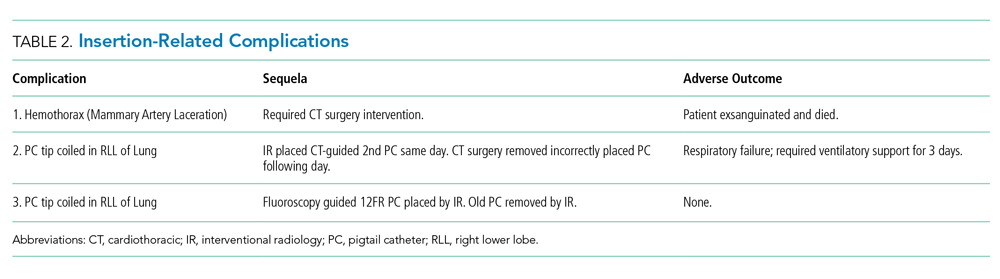
Overall, the AO rate was low. Out of 124 attempted PC placements only 3 (2.4%) had an AO, and as noted above, it is believed that 2 of these patients had an AO caused by other medical problems rather than by PC placement.