Two-Year Experience of 14 French Pigtail Catheters Placed by Procedure-Focused Hospitalists





BACKGROUND: Recent studies show small-bore chest tubes, commonly 14 French pigtail catheters (PCs), are noninferior to large-bore chest tubes for treating various conditions, and they are associated with better patient comfort. The Medical College of Wisconsin implemented a bedside procedure service (BPS) that has been trained in the placement of PCs as an adjunct to its interventional radiology department.
METHODS: The data regarding consults for PC placement was collected by the BPS over a 2-year period. Primary outcomes reviewed were insertion-related complications (IRCs), unsuccessful attempts (UAs), and adverse outcomes (AOs) because the authors believe these represent the safety and effectiveness of the group. It was determined which services consulted the BPS for PC placement, the indications for consults, and a brief review of declined PC consults.
RESULTS: Of the 124 accepted consults, the service had 3 IRCs (2.4%), 2 UAs (1.6%), and 3 AOs (2.4%). A total of 18 consults were declined. The BPS was consulted by 12 services with 8 primary reasons for PC placement.
CONCLUSIONS: At high-volume, tertiary care centers, and with the support of cardiothoracic surgical and interventional radiology services, procedure-focused hospitalists can safely serve as an adjunct service for PC placement in selected hospitalized patients.
© 2020 Society of Hospital Medicine
BPS Operation
Daily BPS operation consists of one attending hospitalist, two internal medicine residents, and a third-year medical student. PCs are placed primarily (95%) by the attending on service under ultrasound guidance using the Seldinger technique with lidocaine for anesthetic. For all PC consults, the attending BPS physician reviews the indication prior to placement. If not a direct consult from surgical services, most PC consults are appropriate referrals to the service after the primary medicine service has consulted CT-surgery or p ulmonary consult teams. After review, the primary role of the BPS is assessing safety of PC placement, including whether the patient can tolerate PC placement without procedural sedation. The BPS’s additional standards for safe PC placement are listed in Table 1.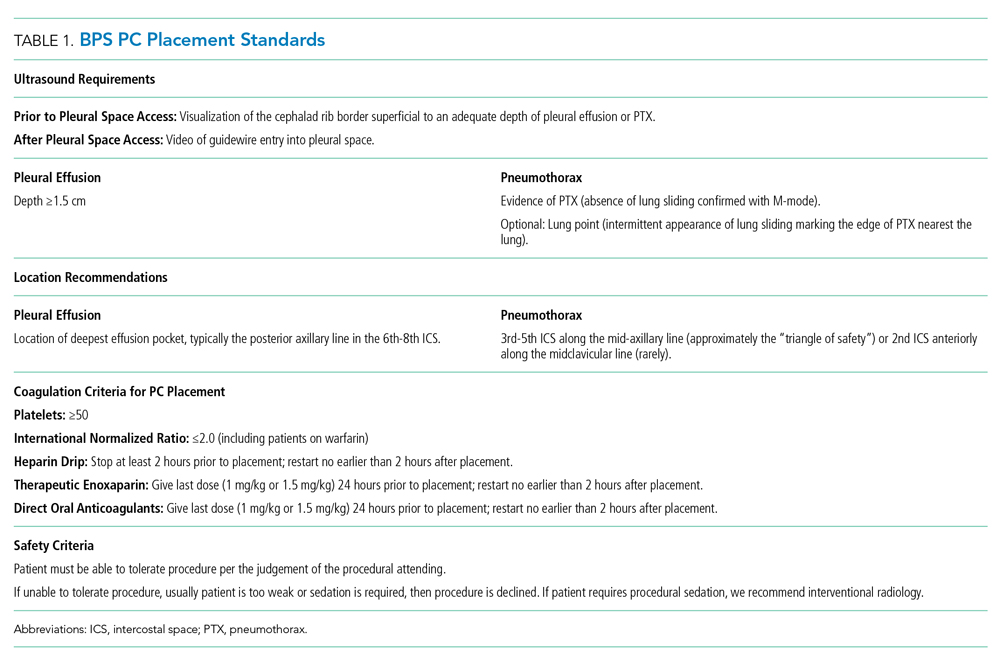
Additionally, it is not routine practice of the BPS to recommend PC placement when consulted for a thoracentesis. The exception to this rule is patients whose PPE sonographic imaging demonstrates loculation or septations. This is consistent with the latest review on pleural disease.13 In addition, the institution’s CT surgery services prefer to initially treat septated PPEs with PCs and fibrinolytic therapy rather than immediate video-assisted thoracoscopic surgery (VATS).
The BPS operates a partnership with CT surgery in which, after successful PC placement, CT surgery manages the PC immediately and until removal including the negative pressure applied and need for fibrinolytic therapy. CT surgery also determines if secondary therapy, commonly second PC or VATS, is required. After PC placement, a portable chest x-ray (CXR) is taken and then BPS follows the patient in person the following day to note any insertion-related complications (IRCs).
In this paper, data on the consults to the BPS for PC placement over a 2-year period are presented. Primary outcomes included numbers of and indications for PCs consulted—attempted or not attempted—consulting services, IRCs, unsuccessful attempts (UAs), and adverse outcomes (AOs). PC duration, fluid drainage, need for fibrinolytic therapy, or need for secondary therapy were not measured because these decisions were managed by the CT surgery service.
PATIENTS AND METHODS
Institutional review board approval of this retrospective study was granted by MCW/Froedtert Hospital Institutional Review Board #5 on January 14, 2019 (MCW IRB #PRO00033496). Adult patients hospitalized at Froedtert Hospital whose primary team determined they would clinically benefit from a PC and consulted the BPS service for placement were included. There were no exclusion criteria.
The authors conducted a retrospective review of two secure BPS databases. The first database is a record of all procedure consults, while the second database contains information about all attempted PCs. Initial review of the BPS’s consult database found 142 PC consults. Consults were classified as “declined” or “attempted.”