Patient Preferences for Physician Attire: A Multicenter Study in Japan





BACKGROUND: Previous studies have shown that patients have specific expectations regarding physician dress. Japan has a cultural background that is in many ways distinct from western countries. Thus, physician attire may have a different impact in Japan.
METHODS: We conducted a multicenter, cross-sectional study to examine patients’ preferences for and perceptions of physician attire in Japan. The questionnaire was developed using photographs of either a male or female physician dressed in seven different forms of attire, and it was randomly distributed to inpatients and outpatients. Respondents were asked to rate the provider pictured; they were also asked to provide preferences for different forms of attire in varied clinical settings. Preference was evaluated for five domains (knowledgeable, trustworthy, caring, approachable, and comfortable). We also assessed variation in preferences for attire by respondent characteristics.
RESULTS: A total of 1,233 (61%) patients indicated that physician dress was important, and 950 (47%) patients agreed that it influenced their satisfaction with care. Compared with all forms, casual attire with a white coat was the most preferred dress. Older patients more often preferred formal attire with a white coat in primary care and hospital settings. In addition, physician attire had a greater impact on older respondents’ satisfaction and experience.
CONCLUSION: The majority of Japanese patients indicated that physician attire is important and influenced their satisfaction with care. Geography, settings of care, and patient age appear to play a role in patient preferences.
© 2020 Society of Hospital Medicine
Questionnaires were printed and randomly distributed by research staff to outpatients in waiting rooms and inpatients in medical wards who were 20 years of age or older. We placed no restriction on ward site or time of questionnaire distribution. Research staff, including physicians, nurses, and medical clerks, were instructed to avoid guiding or influencing participants’ responses. Informed consent was obtained by the staff; only those who provided informed consent participated in the study. Respondents could request assistance with form completion from persons accompanying them if they had difficulties, such as physical, visual, or hearing impairments. All responses were collected anonymously. The study was approved by the ethics committees of all four hospitals.
Questionnaire
We used a modified version of the survey instrument from a prior study.10 The first section of the survey showed photographs of either a male or female physician with 7 unique forms of attire, including casual, casual with white coat, scrubs, scrubs with white coat, formal, formal with white coat, and business suit (Figure 1). Given the Japanese context of this study, the language was translated to Japanese and photographs of physicians of Japanese descent were used. Photographs were taken with attention paid to achieving constant facial expressions on the physicians as well as in other visual cues (eg, lighting, background, pose). The physician’s gender and attire in the first photograph seen by each respondent were randomized to prevent bias in ordering, priming, and anchoring; all other sections of the survey were identical.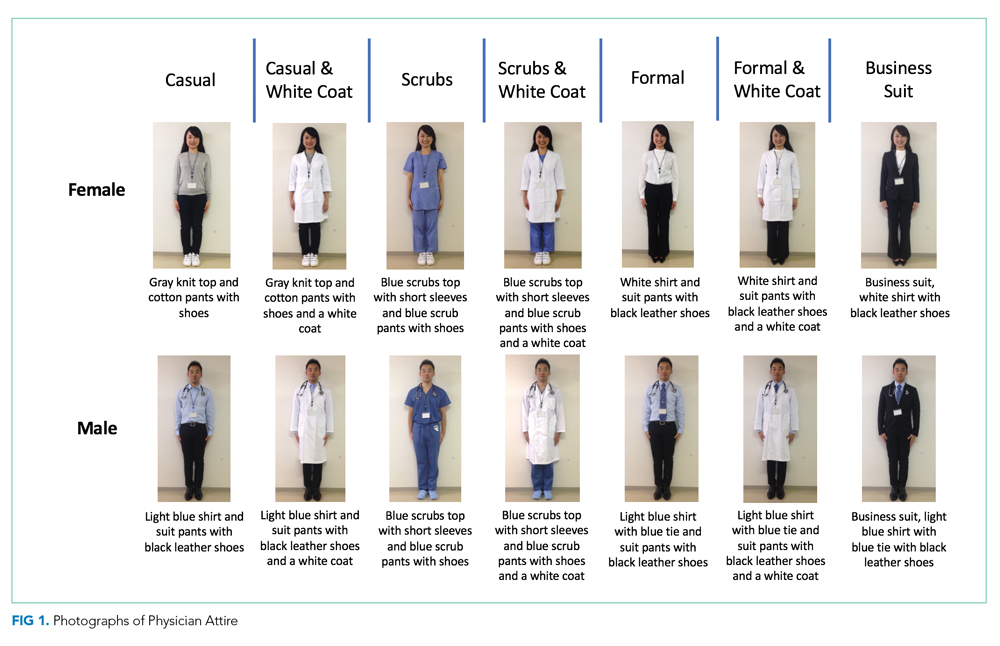
Respondents were first asked to rate the standalone, randomized physician photograph using a 1-10 scale across five domains (ie, how knowledgeable, trustworthy, caring, and approachable the physician appeared and how comfortable the physician’s appearance made the respondent feel), with a score of 10 representing the highest rating. Respondents were subsequently given 7 photographs of the same physician wearing various forms of attire. Questions were asked regarding preference of attire in varied clinical settings (ie, primary care, ED, hospital, surgery, overall preference). To identify the influence of and respondent preferences for physician dress and white coats, a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree) was employed. The scale was trichotomized into “disagree” (1, 2), “neither agree nor disagree” (3), and “agree” (4, 5) for analysis. Demographic data, including age, gender, education level, nationality (Japanese or non-Japanese), and number of physicians seen in the past year were collected.
Outcomes and Sample Size Calculation
The primary outcome of attire preference was calculated as the mean composite score of the five individual rating domains (ie, knowledgeable, trustworthy, caring, approachable, and comfortable), with the highest score representing the most preferred form of attire. We also assessed variation in preferences for physician attire by respondent characteristics, such as age and gender.
Sample size estimation was based on previous survey methodology.10 The Likert scale range for identifying influence of and respondent preferences for physician dress and white coats was 1-5 (“strongly disagree” to “strongly agree”). The scale range for measuring preferences for the randomized attire photograph was 1-10. An assumption of normality was made regarding responses on the 1-10 scale. An estimated standard deviation of 2.2 was assumed, based on prior findings.10 Based on these assumptions and the inclusion of at least 816 respondents (assuming a two-sided alpha error of 0.05), we expected to have 90% capacity to detect differences for effect sizes of 0.50 on the 1-10 scale.