Decreasing Hypoglycemia following Insulin Administration for Inpatient Hyperkalemia





BACKGROUND: Acute hyperkalemia (serum potassium ≥ 5.1 mEq/L) is often treated with a bolus of IV insulin. This treatment may result in iatrogenic hypoglycemia (glucose < 70 mg/dl).
OBJECTIVES: The aims of this study were to accurately determine the frequency of iatrogenic hypoglycemia following insulin treatment for hyperkalemia, and to develop an electronic health record (EHR) orderset to decrease the risk for iatrogenic hypoglycemia.
DESIGN: This study was an observational, prospective study.
SETTING: The setting for this study was a university hospital.
PATIENTS: All nonobstetric adult inpatients in all acute and intensive care units were eligible.
INTERVENTION: Implementation of a hyperkalemia orderset (Orderset 1.1) with glucose checks before and then one, two, four, and six hours after regular intravenous insulin administration. Based on the results from Orderset 1.1, Orderset 1.2 was developed and introduced to include weight-based dosing of insulin options, alerts identifying patients at higher risk of hypoglycemia, and tools to guide decision-making based on the preinsulin blood glucose level.
MEASUREMENTS: Patient demographics, weight, diabetes history, potassium level, renal function, and glucose levels were recorded before, and then glucose levels were measured again at one, two, four, and six hours after insulin was administered.
RESULTS: The iatrogenic hypoglycemia rate identified with mandatory glucose checks in Orderset 1.1 was 21%; 92% of these occurred within three hours posttreatment. Risk factors for hypoglycemia included decreased renal function (serum creatinine >2.5 mg/dl), a high dose of insulin (>0.14 units/kg), and re-treatment with blood glucose < 140 mg/dl. After the introduction of Orderset 1.2, the rate of iatrogenic hypoglycemia decreased to 10%.
CONCLUSIONS: The use of an EHR orderset for treating hyperkalemia may reduce the risk of iatrogenic hypoglycemia in patients receiving insulin while still adequately lowering their potassium.
© 2020 Society of Hospital Medicine
Additionally, we explored the frequency in which providers ordered insulin through the hyperkalemia orderset for each version of the orderset via two-month baseline reviews. Investigation for Orderset 1.1 was from January 1, 2017 to February 28, 2017 and for Orderset 1.2 was from August 1, 2017 to September 30, 2017. Insulin ordering frequency through the hyperkalemia orderset was defined as ordering insulin through the adult inpatient hyperkalemia orderset versus ordering insulin in and outside of the hyperkalemia orderset.
Last, we measured the nursing point of care testing (POCT) blood glucose measurement compliance with the hyperkalemia orderset. Nursing utilization acceptance of the hyperkalemia orderset was defined as adequate POCT blood glucose levels monitored in comparison to all insulin treatments via the hyperkalemia orderset.
Setting and Participants
We evaluated nonobstetric adult inpatients admitted to UCSF Medical Center between January 2016 and September 2017. All medical and surgical wards and intensive care units were included in the analysis.
Intervention
In June 2012, an EHR developed by Epic Systems was introduced at UCSFMC. In January 2016, we designed a new EHR-based hyperkalemia treatment orderset (Orderset 1.1), which added standard POCT blood glucose checks before and at one, two, four, and six hours after insulin injection (Appendix 1). In March 2017, a newly designed orderset (Orderset 1.2) replaced the previous hyperkalemia treatment orderset (Appendix 2). Orderset 1.2 included three updates. First, providers were now presented the option of ordering insulin as a
CORRECTED FIGURE PER ERRATUM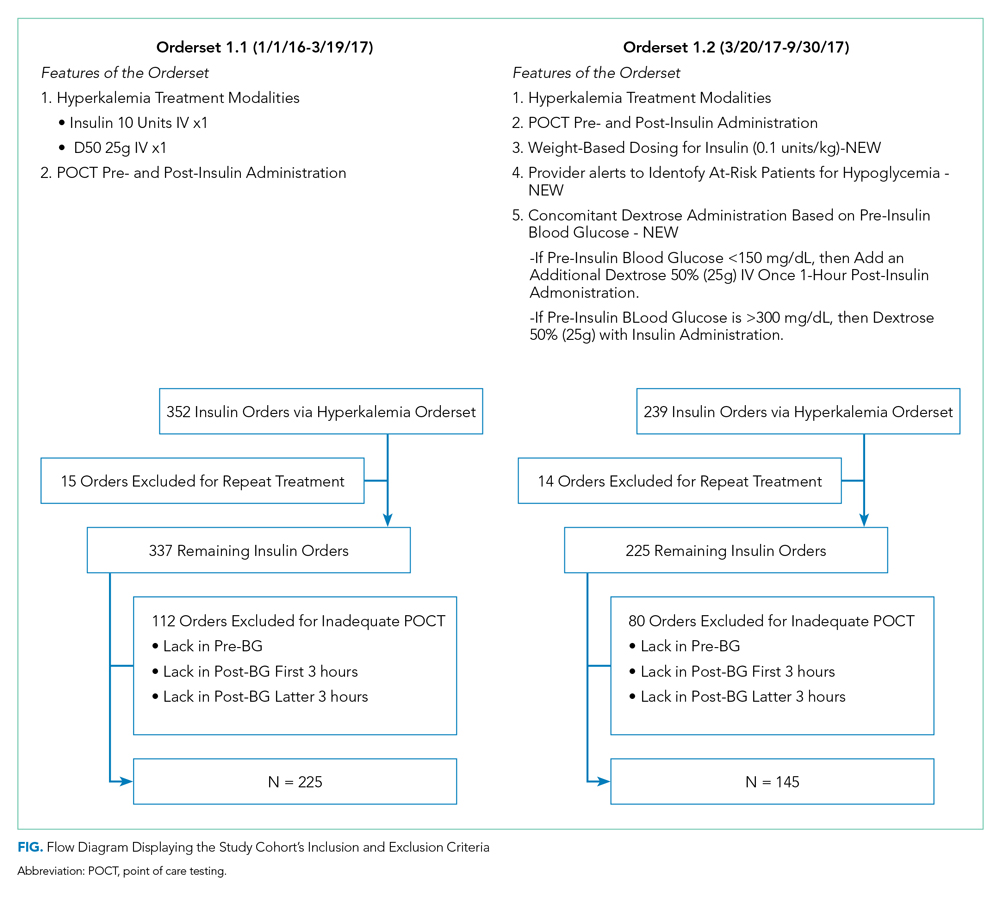
Inclusion and exclusion criteria are shown in the Figure. All patients who had insulin ordered via a hyperkalemia orderset were included in an intention-to-treat analysis. A further analysis was performed for patients for whom orderset compliance was achieved (ie, insulin ordered through the ordersets with adequate blood glucose monitoring). These patients were required to have a POCT blood glucose check preinsulin administration and postinsulin administration as follows: (1) between 30 to 180 minutes (0.5 to three hours) after insulin administration, and (2) between 180 and 360 minutes (three to six hours) after insulin administration. For patients receiving repeated insulin treatments for hyperkalemia within six hours, the first treatment data points were excluded to prevent duplication.
Outcomes
We extracted data on all nonobstetric adult patients admitted to UCSFMC between January 1, 2016 and March 19, 2017 (Orderset 1.1) and between March 20, 2017 and September 30, 2017 (Orderset 1.2).
We measured unique insulin administrations given that each insulin injection poses a risk of iatrogenic hypoglycemia. Hypoglycemia was defined as glucose <70 mg/dL and severe hypoglycemia was defined as glucose <40 mg/dL. Covariates included time and date of insulin administration; blood glucose levels before and at one, two, four, and six hours after insulin injection (if available); sex; weight; dose of insulin given for hyperkalemia treatment; creatinine; known diagnosis of diabetes; concomitant use of albuterol; and concomitant use of corticosteroids. Hyperglycemia was defined as glucose >180 mg/dL. We collected potassium levels pre- and postinsulin treatment. The responsible team’s discipline and the location of the patient (eg, medical/surgical unit, intensive care unit, emergency department) where the insulin orderset was used were recorded.
