High-Flow Nasal Cannula Oxygen in Patients with Acute Respiratory Failure and Do-Not-Intubate or Do-Not-Resuscitate Orders: A Systematic Review





BACKGROUND AND OBJECTIVES: High-flow nasal cannula (HFNC) oxygen may provide tailored benefits in patients with preset treatment limitations. The objective of this study was to assess the effectiveness of HFNC oxygen in patients with do-not-intubate (DNI) and/or do-not-resuscitate (DNR) orders.
METHODS: We conducted a systematic review of interventional and observational studies. A search was performed using MEDLINE, EMBASE, CINAHL, Scopus, and Web of Science, from inception to October 15, 2018.
RESULTS: We included six studies evaluating 293 patients. All studies had a high risk of bias. The hospital mortality rates of patients with DNI and/or DNR orders receiving HFNC oxygen were variable and ranged from 40% to 87%. In two before and after studies, the initiation of HFNC oxygen was associated with improved oxygenation and reduced respiratory rates. One comparative study found no difference in dyspnea reduction or morphine doses between patients using HFNC oxygen versus conventional oxygen. No studies evaluated quality of life in survivors or quality of death in nonsurvivors. HFNC was generally well tolerated with few adverse events identified.
CONCLUSIONS: While HFNC oxygen remains a viable treatment option for hospitalized patients who have acute respiratory failure and a DNI and/or DNR order, there is a paucity of high-quality, comparative, effectiveness data to guide the usage of HFNC oxygen compared with other treatments, such as noninvasive ventilation, conventional oxygen, and palliative opioids.
© 2019 Society of Hospital Medicine
Mortality
The hospital mortality rates of patients with DNI and/or DNR orders receiving HFNC were variable and ranged from 40% to 87%. In the two studies enrolling general ICU patient populations, the hospital mortality rates ranged from 40% to 60%. In the four studies enrolling patients with active malignancy, the hospital mortality rates ranged from 75% to 87%. No studies compared mortality rates with and without DNI and/or DNR orders.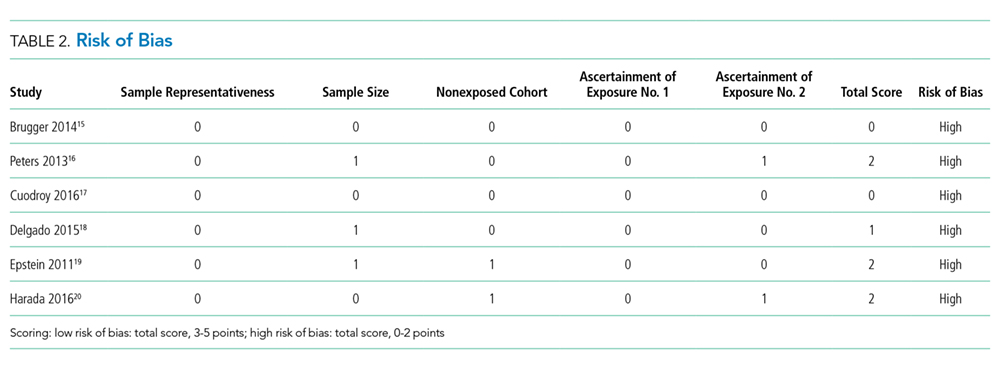
Dyspnea, Work of Breathing, and Reduction in Opioid Doses
The impact of HFNC oxygen on symptom relief was reported in one retrospective observational study (published as a conference abstract only to date), which compared the effect of HFNC oxygen (n = 101) with conventional oxygen (n = 110).18 At first evaluation after hospital admission to a palliative care unit (after the patients had previously been started on either conventional oxygen or high-flow oxygen), patients in the HFNC oxygen group had worse (higher) dyspnea scores compared with patients who used conventional oxygen (Edmonton Symptom Assessment Scale score of 7.5 versus 5, P < .001). At follow-up, approximately 24 hours after admission to the hospital palliative care unit, there was no difference in the change of dyspnea between the HFNC oxygen group (dyspnea score change of 0) and the conventional oxygen group (dyspnea score change of −1, P = .18. In the same study, there was also no significant difference in the morphine dose requirement in each group, and exact doses were not reported.
Two studies reported improvement in oxygen saturation and respiratory rate after HFNC oxygen initiation (compared with before HFNC initiation).16,20 Oxygen saturation increased from 89% to 95%, P < .01, in one study and 92% to 97%, P < .01, in a second study. The respiratory rate decreased from 31 to 25 breaths/minute in one study, and from 28 to 25 breaths/minute in a second study (both P < .01).
Quality of Life
No studies evaluated the quality of life of survivors.
Secondary Outcomes
Transition to Noninvasive Positive Pressure Ventilation
The proportion of patients who transitioned from HFNC oxygen to NPPV was relatively low in the two studies that reported this outcome, ranging from 0%20 to 18%.16 In one observational study of a general ICU population, 9/50 (18%) of patients transitioned from HFNC oxygen to NPPV. There was no statistically significant difference in hospital mortality rates among those who progressed to NPPV (67%) versus those who did not progress to NPPV (58%), P = .72.
Tolerance of HFNC and Adverse Events
HFNC oxygen was generally well tolerated based on the assessment of three studies (Table 1). One study reported no adverse events,16 one study reported that HFNC oxygen had to be discontinued because of nasal discomfort in 1% of patients,19 and a second study reported that HFNC oxygen had to be discontinued because of agitation in 4% of patients.20
Quality of Death in Nonsurvivors
No studies evaluated the quality of death in those patients who died.
