High-Flow Nasal Cannula Oxygen in Patients with Acute Respiratory Failure and Do-Not-Intubate or Do-Not-Resuscitate Orders: A Systematic Review





BACKGROUND AND OBJECTIVES: High-flow nasal cannula (HFNC) oxygen may provide tailored benefits in patients with preset treatment limitations. The objective of this study was to assess the effectiveness of HFNC oxygen in patients with do-not-intubate (DNI) and/or do-not-resuscitate (DNR) orders.
METHODS: We conducted a systematic review of interventional and observational studies. A search was performed using MEDLINE, EMBASE, CINAHL, Scopus, and Web of Science, from inception to October 15, 2018.
RESULTS: We included six studies evaluating 293 patients. All studies had a high risk of bias. The hospital mortality rates of patients with DNI and/or DNR orders receiving HFNC oxygen were variable and ranged from 40% to 87%. In two before and after studies, the initiation of HFNC oxygen was associated with improved oxygenation and reduced respiratory rates. One comparative study found no difference in dyspnea reduction or morphine doses between patients using HFNC oxygen versus conventional oxygen. No studies evaluated quality of life in survivors or quality of death in nonsurvivors. HFNC was generally well tolerated with few adverse events identified.
CONCLUSIONS: While HFNC oxygen remains a viable treatment option for hospitalized patients who have acute respiratory failure and a DNI and/or DNR order, there is a paucity of high-quality, comparative, effectiveness data to guide the usage of HFNC oxygen compared with other treatments, such as noninvasive ventilation, conventional oxygen, and palliative opioids.
© 2019 Society of Hospital Medicine
METHODS
We conducted a systematic review of studies that evaluated patients who used HFNC oxygen for acute respiratory failure and had a DNI and/or DNR order. We reported the results using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements.13 This review was registered with the PROSPERO registry, CRD42017059914.
We included studies that enrolled patients who were (1) hospitalized, (2) >18 years old, (3) had an acute respiratory failure of any cause, (4) received HFNC oxygen, and (5) had a DNI or DNR or comfort measures only order. We included publications of all study designs (interventional, observational, and posthoc analyses) and all languages. We excluded studies that enrolled <5 patients. If necessary, we contacted the authors of the included studies for additional information.
Our search strategy included the following databases from inception to October 14, 2018: PubMed, MEDLINE, CINAHL, MICROMEDEX, EMBASE, Web of Science, and Scopus. The database-specific search strategy was developed using an experienced librarian (Appendix Table 2). In addition, we screened the reference lists of systematic reviews as well as the included studies to find additional relevant articles. Two authors (AM, MEW) independently assessed the inclusion criteria of the titles and abstracts that were identified in the search. In addition, these two authors abstracted relevant data of the included studies.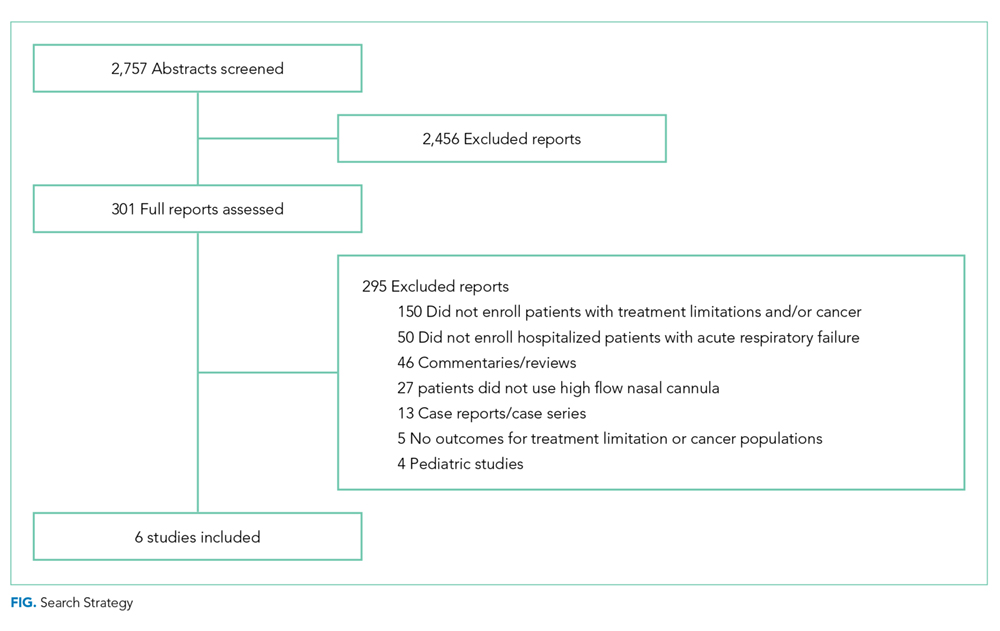
The primary outcomes were mortality, dyspnea and work of breathing, quality of life, and reduction of opioid doses. Secondary, posthoc, outcomes included the transition to noninvasive positive pressure ventilation (NPPV), tolerance of HFNC, adverse events, and quality of death in nonsurvivors. The risk of bias was evaluated using a modified Newcastle-Ottawa Quality Assessment Scale (Appendix Table 3).
RESULTS
Using the search strategy, we identified 2,757 citations and included 301 of these in the full-text review (Figure). We included six studies, which enrolled 293 patients in the final systematic review. Table 1 summarizes the characteristics of the included investigations, all of which were observational studies.15-20 The studies were conducted in the United States of America (n = 3), Europe (n = 2), and Asia (n = 1). Two studies were conducted in the general ICU populations and included patients with hypoxemic respiratory failure only. Four studies were conducted in cancer populations in the hospital wards or ICU and did not specify the type of respiratory failure (hypoxemic versus hypercapnic). Two studies included patients with DNI orders only.15,20 One study included patients with DNR orders only (DNI orders were excluded).17 Three studies included patients with both DNR and DNI orders.16,18,19 The numbers of enrolled patients with treatment limitations were generally low, with the two largest studies including 101 patients each on HFNC oxygen.18,19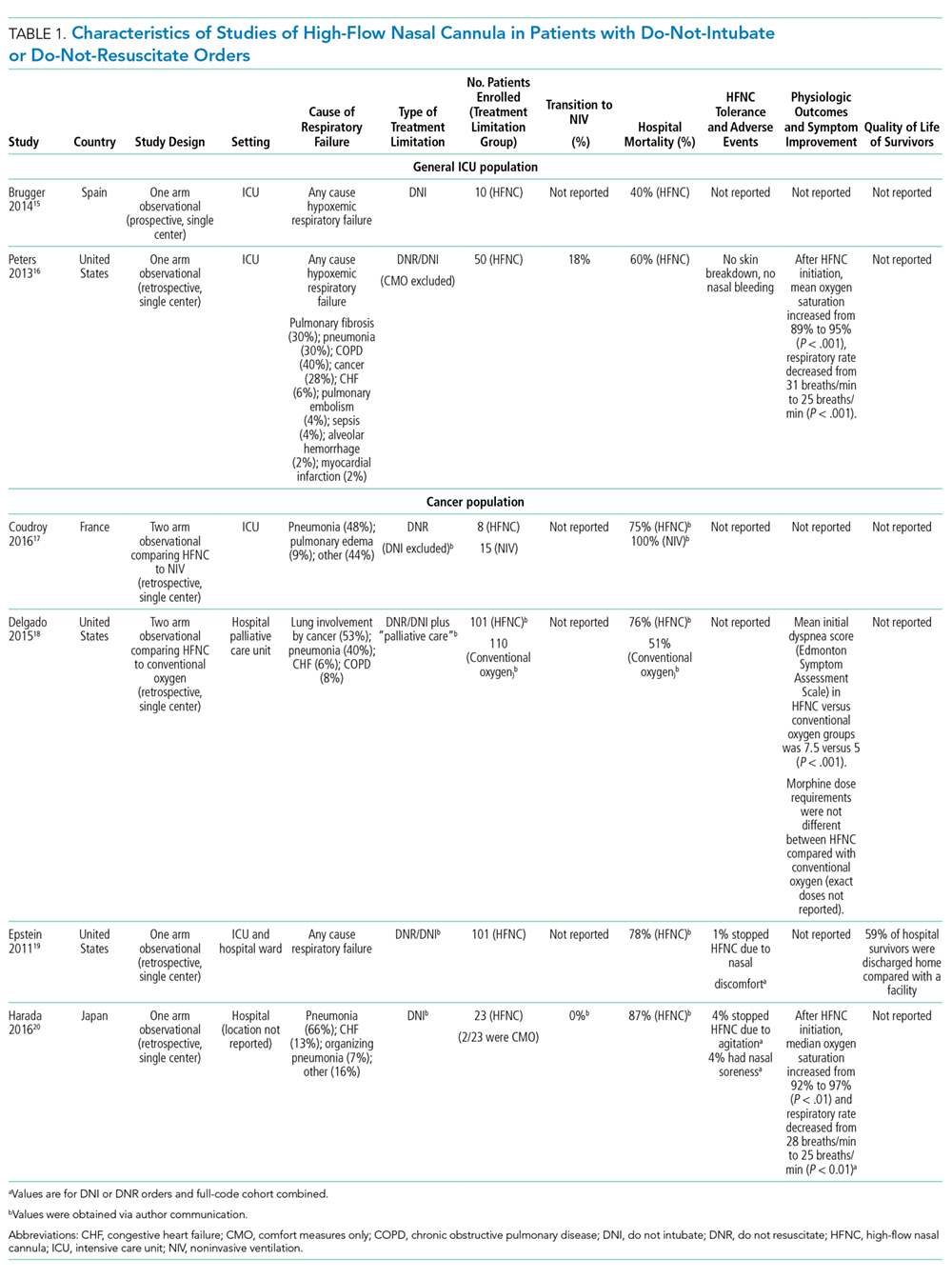
Risk of Bias
All included studies had a high risk of bias (Table 2). A high risk of bias was suggested because the investigations were single-center studies with unclear patient selection methods, did not explicitly report how decisions to limit treatments were made, and did not explicitly differentiate and separately analyze patients with “comfort measures only” goals of care.
