Does Scheduling a Postdischarge Visit with a Primary Care Physician Increase Rates of Follow-up and Decrease Readmissions?





BACKGROUND: Driven in part by Medicare’s Hospital Readmissions Reduction Program, hospitals are focusing on improving the transition from inpatient to outpatient care with particular emphasis on early follow-up with a primary care physician (PCP).
OBJECTIVE: To assess whether the implementation of a scheduling assistance program changes rates of PCP follow-up or readmissions. DESIGN: Retrospective cohort study.
SETTING: An urban tertiary care center
PATIENTS: A total of 20,918 adult patients hospitalized and discharged home between September 2008 and October 2015.
INTERVENTION: A postdischarge appointment service to facilitate early PCP follow-up.
MAIN MEASURES: Primary outcomes were rates of follow-up visits with a PCP within seven days of discharge and hospital readmission within 30 days of discharge. Our first analysis assessed differences in outcomes among patients with and without the use of the service. In a second analysis, we exploited the fact that the service was not available on weekends and conducted an instrumental variable analysis that used the interaction between the intervention and day of the week of admission.
RESULTS: In our multivariable analysis, use of the appointment service was associated with much higher rates of PCP follow-up (+31.9 percentage points, 95% CI: 30.2, 33.6; P < .01) and a decrease in readmission (−3.8 percentage points, 95% CI: −5.2, −2.4; P < .01). In the instrumental variable analysis, use of the service also increased the likelihood of a PCP follow-up visit (33.4 percentage points, 95% CI: 7.9, 58.9; P = .01) but had no significant impact on readmissions (−2.5 percentage points, 95% CI: −22.0, 17.0; P = .80).
CONCLUSIONS: The postdischarge appointment service resulted in a substantial increase in timely PCP follow-up, but its impact on the readmission rate was less clear.
© 2019 Society of Hospital Medicine
RESULTS
Overall, there were 17,582 hospitalizations on the medicine and cardiology services following implementation of the postdischarge appointment service. The use of the postdischarge appointment service rose rapidly after it was introduced (Figure) and then plateaued at roughly 50%. 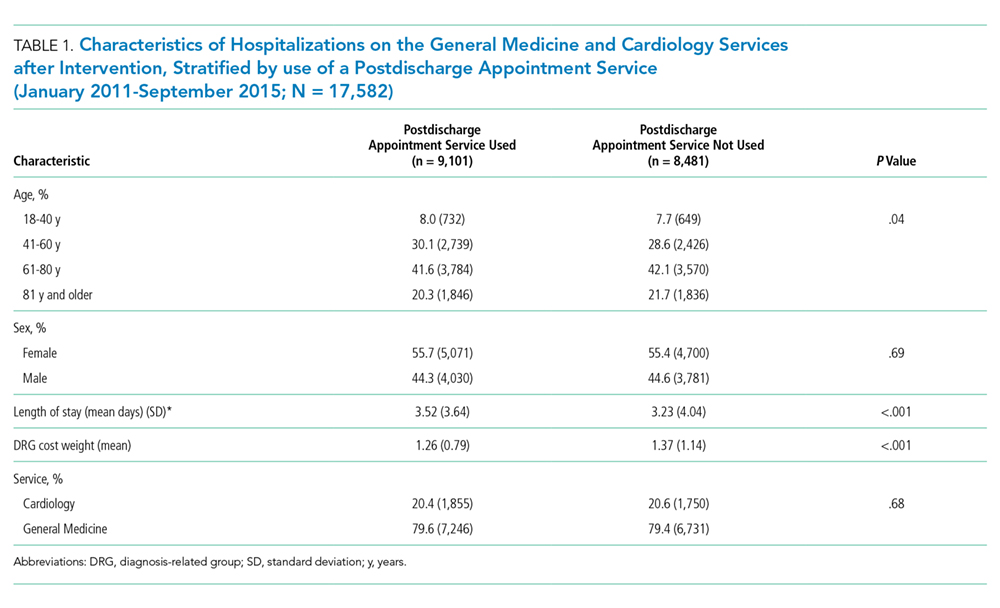
Multivariable Logistic Regression
In this analysis, we focused on the 17,582 hospitalizations from January 2011 to September 2015 on the general medicine and cardiology services that occurred after the postdischarge appointment service was introduced. Among these hospitalizations, the postdischarge appointment service was used in 51.8% of discharges.
In an unadjusted analysis, patients discharged using the tool had higher rates of seven-day PCP follow-up (60.2% vs 29.2%, P < .001) and lower 30-day readmission rates (14.7% vs 16.7%; P < .001) than those who were not (Table 2). There was no significant difference in 30-day ED revisit between hospitalizations with and without use of the postdischarge appointment service (22.3% vs 23.1%; P = .23).
This was echoed in our multivariable analysis where, controlling for other patient factors, use of the postdischarge appointment service was associated with an increased rate of follow-up with a PCP in seven days (+31.9 percentage points; 95% CI: 30.2, 33.6; P < .01) and a decreased likelihood of readmission within 30 days (−3.8 percentage points; 95% CI: −5.2, −2.4; P < .01) (Table 2).
Instrumental Variable Analysis
In our instrumental variable analysis, we used all hospitalizations both before and after the introduction of the intervention. In this analysis, we estimate that use of the postdischarge appointment service increases the probability of visiting a PCP within seven days by 33.4 percentage points (95% CI: 7.9%, 58.9%; P = .01) (Table 3). The use of the postdischarge appointment was associated with a 2.5 percentage point (95% CI: −22.0%, 17.1%; P = .80) reduction in readmissions and a 4.8 percentage point (95% CI; −27.5%, 17.9%; P = .68) reduction in an ED visit within 30 days (Table 3). Neither of these differences were statistically significant with wide confidence intervals.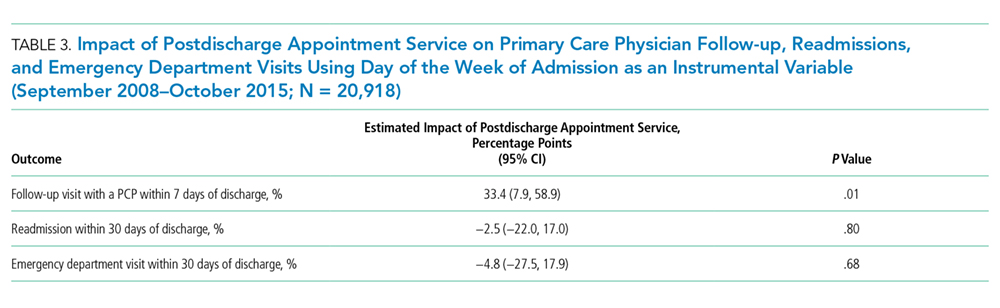
In sensitivity analyses, we obtained similar results when we considered PCP visits and readmissions within 14 days.
DISCUSSION
The hospital introduced the postdischarge appointment service to facilitate postdischarge appointments and to deter readmissions. In our analyses the use of the postdischarge appointment service was associated with a substantial 30 percentage point increase in the likelihood of a PCP follow-up visit within seven days after hospital discharge. There was a roughly 2% reduction in 30-day readmissions, but this difference was not consistently statistically significant across our analyses. Together, our evaluation implies that this type of intervention may make it much easier for patients to attend a PCP appointment, but scheduling an appointment alone may have a modest impact on deterring a readmission.
