Does Scheduling a Postdischarge Visit with a Primary Care Physician Increase Rates of Follow-up and Decrease Readmissions?





BACKGROUND: Driven in part by Medicare’s Hospital Readmissions Reduction Program, hospitals are focusing on improving the transition from inpatient to outpatient care with particular emphasis on early follow-up with a primary care physician (PCP).
OBJECTIVE: To assess whether the implementation of a scheduling assistance program changes rates of PCP follow-up or readmissions. DESIGN: Retrospective cohort study.
SETTING: An urban tertiary care center
PATIENTS: A total of 20,918 adult patients hospitalized and discharged home between September 2008 and October 2015.
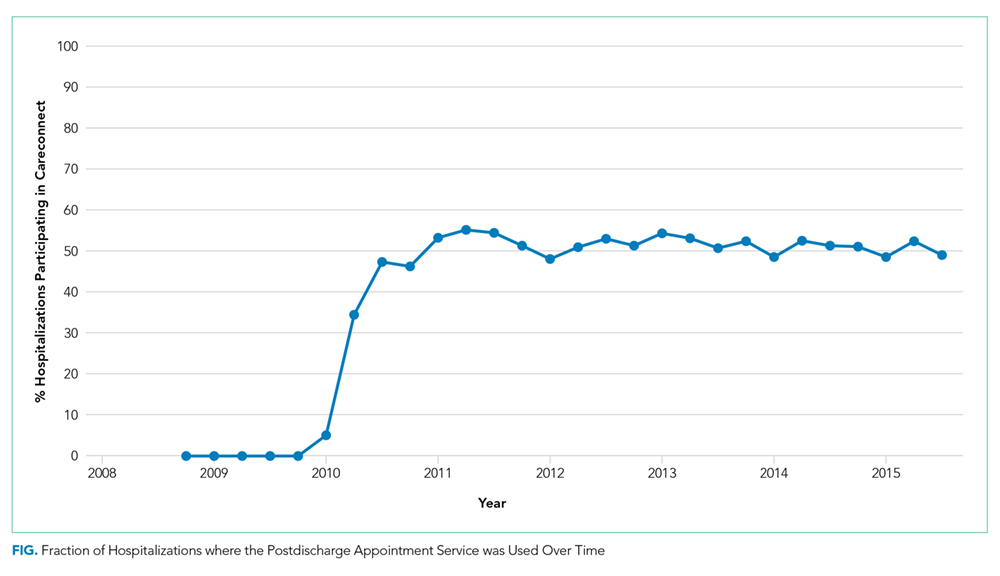
INTERVENTION: A postdischarge appointment service to facilitate early PCP follow-up.
MAIN MEASURES: Primary outcomes were rates of follow-up visits with a PCP within seven days of discharge and hospital readmission within 30 days of discharge. Our first analysis assessed differences in outcomes among patients with and without the use of the service. In a second analysis, we exploited the fact that the service was not available on weekends and conducted an instrumental variable analysis that used the interaction between the intervention and day of the week of admission.
RESULTS: In our multivariable analysis, use of the appointment service was associated with much higher rates of PCP follow-up (+31.9 percentage points, 95% CI: 30.2, 33.6; P < .01) and a decrease in readmission (−3.8 percentage points, 95% CI: −5.2, −2.4; P < .01). In the instrumental variable analysis, use of the service also increased the likelihood of a PCP follow-up visit (33.4 percentage points, 95% CI: 7.9, 58.9; P = .01) but had no significant impact on readmissions (−2.5 percentage points, 95% CI: −22.0, 17.0; P = .80).
CONCLUSIONS: The postdischarge appointment service resulted in a substantial increase in timely PCP follow-up, but its impact on the readmission rate was less clear.
© 2019 Society of Hospital Medicine
Study Population
We conducted a retrospective, cohort study at Beth Israel Deaconess Medical Center, a tertiary care hospital, using data derived from electronic health records for all hospitalizations
Outcomes
The primary outcomes of this study were kept PCP follow-up visits within seven days and readmission within 30 days of discharge. We focused on PCP visits within seven days, as this has been the measure used in prior research,5,7 but conducted a sensitivity analysis of PCP follow-up within 14 days. No-shows for the scheduled follow-up PCP appointments were not included. We focused on readmissions within 30 days of discharge, given this is the measure used in the HRRP,16 but conducted a sensitivity analysis of 14 days. Secondary outcomes included ED revisit within the 30 days. Given the data available, we only observed physician visits and hospitalizations that occurred within the Beth Israel Deaconess system.
Analyses
We conducted two analyses to assess whether the implementation of the postdischarge appointment service was associated with an increase in PCP follow-up and a decrease in the readmission rate.
In the first analysis, we focused only on hospitalizations from the medical and cardiology services during the postintervention period between January 2011 and September 2015 (n = 17,582). We compared the PCP follow-up rate and the readmission rate among hospitalizations where the postdischarge appointment service was used versus those where it was not used. We used a multivariable logistic regression, and the covariates included in the model were age, gender, hospital length of stay, and diagnosis-related group (DRG) cost weight. The DRG cost weight captures the average resources used to treat Medicare patients’ hospitalizations within a given DRG category and was used as a surrogate marker for the complexity of hospitalization.17 Instead of presenting odds ratios, we used predictive margins to generate adjusted percentage point estimates of the differences in our outcomes associated with the use of the postdischarge appointment service.18
This instrumental variable exploits the fact that the postdischarge appointment service was only available on weekdays and that physicians are asked to only submit the order for follow-up appointments on the day of discharge. We focused on the day of the week of admission (versus discharge) because of concerns that patients with more complicated hospital courses might be kept in the hospital over the weekend (eg, to facilitate testing available only on weekdays or to consult with regular physicians only available on weekdays). This would create a relationship between the day of discharge and the outcomes (follow-up visits, readmissions). The day of admission is less likely to be impacted by this bias. Given concerns that admissions on different days of the week might be different, our instrument is the day of the week interacted with the time period. Therefore, to create bias, there must be a systematic change in the nature of admissions on a given day of the week during this time period. We provide more details on this analysis, testing of the instrument, and results in the Appendix.
Analyses were conducted in Stata, version 14.2 (StataCorp LP, College Station, Texas). Statistical testing was two-sided, with a significance level of 0.05, and the project was judged exempt by the Committee on Clinical Investigations for Beth Israel Deaconess Medical Center.