Impact of the Hospital-Acquired Conditions Initiative on Falls and Physical Restraints: A Longitudinal Study





BACKGROUND: The Centers for Medicare & Medicaid Services (CMS) implemented the Hospital-Acquired Conditions (HACs) Initiative in October 2008; the CMS no longer reimbursed hospitals for fall injury. The effects of this payment change on fall and fall injury rates are not well described, nor its effect on physical restraint use.
OBJECTIVE: The aim of this study was to examine the effects of the 2008 HACs Initiative on the rates of falls, injurious falls, and physical restraint use.
DESIGN/SETTING: This was a nine-year retrospective cohort study (July 2006-December 2015) involving 2,862 adult medical, medical-surgical, and surgical nursing units from 734 hospitals.
MEASUREMENTS: Annual rates of change in falls, injurious falls, and physical restraint use during the two years before the payment rule went into effect were compared with one-, four-, and seven-year rates of annual change after implementation, adjusting for unit- and facility-level covariates. Stratified analyses were conducted according to bed size and teaching status.
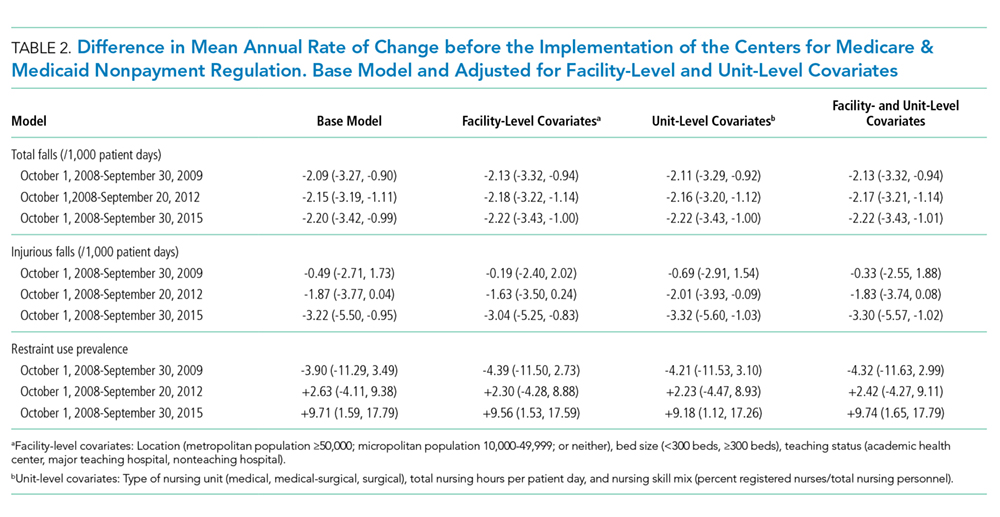
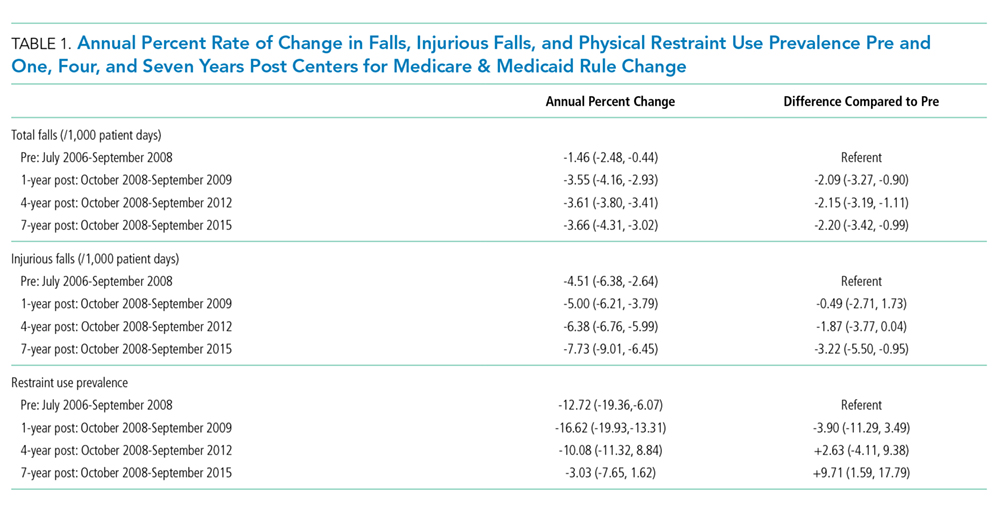
RESULTS: Compared with prior to the payment change, there was stable acceleration in the one-, four-, and seven-year annual rates of decline in falls as follows: -2.1% (-3.3%, -0.9%), -2.2% (-3.2%, -1.1%), and -2.2% (-3.4%, -1.0%) respectively. For injurious falls, there was an increasing acceleration in the annual declines, achieving statistical significance only at seven years post CMS change as follows: -3.2% (-5.5%, -1.0%). Physical restraint use prevalence decreased from 1.6% to 0.6%. Changes in the rates of falls, injurious falls, and restraint use varied according to hospital bed size and teaching status.
CONCLUSIONS AND RELEVANCE: Since the HACs Initiative, there was at best a modest decline in the rates of falls and injurious falls observed primarily in larger, major teaching hospitals. An increase in restraint use was not observed. Falls remain a difficult patient safety problem for hospitals, and further research is required to develop cost-effective, generalizable strategies for their prevention.
© 2019 Society of Hospital Medicine
Baseline Characteristics
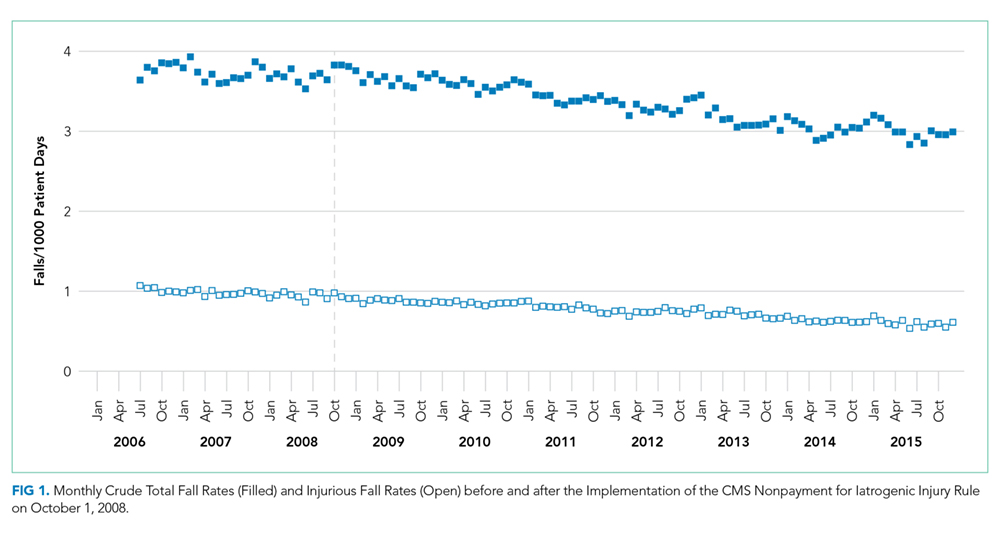
In the first study month (July 2006), 1,941 sample nursing units reported 5,101 falls during 1,401,652 patient-days of observation. Of these, 1,502 (29%) resulted in injury (1,281 minor, 144 moderate, 75 major, and two deaths). Across falls, the median (interquartile range [IQR]) patient age was 70 (55-80) years, with males accounting for 51% of falls. Most of the falls, 4,328 (85%), were documented as unassisted. A total of 209 (4%) falls occurred while physical restraints were in use.
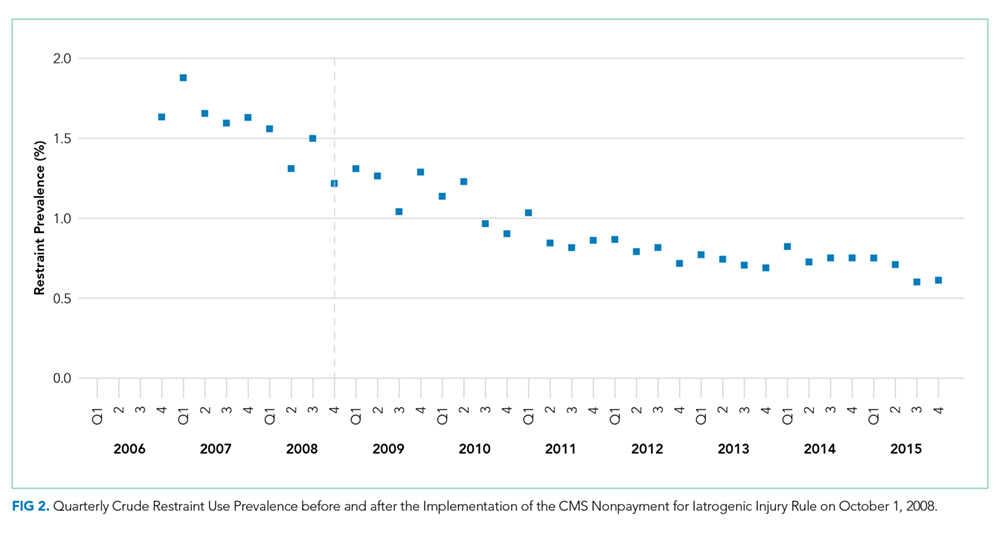
In the first quarterly restraint use prevalence survey (October 2006), the 829 participating nursing units surveyed 19,979 patients (median [IQR] = 23 [20-23] patients per nursing unit). The median (IQR) age was 66 (51-78) years, and 54% of them were females. At the time of the survey, restraints were in use for 326 (1.6%) patients. Restrained patients were older than unrestrained patients (median age: 78 vs 65 years) and more likely to be male (56% vs 46%). Limb restraints were used for 139 patients, vest restraints for 66, both limb and vest restraints for 24, and other restraint types were used for 113 patients (including 11 in limb restraints and 5 in limb and vest restraints).
Change in Endpoints after Implementation of the HACs Initiative
Stratified Analysis
At baseline, fall rates and restraint use prevalence were slightly higher, whereas the rate of injurious falls was slightly lower, among teaching and academic medical centers compared to those in nonteaching hospitals. Declines in falls rate and restraint use prevalence were higher in teaching hospitals than in nonteaching hospitals (data not included).