Quality and Safety of Pediatric Inpatient Care in Community Hospitals: A Scoping Review





BACKGROUND: Although the majority of children are hospitalized in nonchildren's hospitals, little is known about the quality and safety of pediatric care in community hospitals.
OBJECTIVE: The aim of this study was to conduct a scoping review and synthesize literature on the quality and safety of pediatric inpatient care in United States community hospitals.
METHODS: We performed a systematic literature search in October 2016 to identify pediatric studies that reported on safety, effectiveness, efficiency, timeliness, patient-centeredness, or equity set in general, nonuniversity, or nonchildren’s hospitals. We extracted data on study design, patient descriptors, and quality outcomes and assessed the risk of bias using modified Newcastle-Ottawa Scales.
RESULTS: A total of 44 articles met the inclusion criteria. Study designs, patient populations, and quality outcome measures were heterogeneous; only three clinical domains, (1) perinatal regionalization, (2) telemedicine, and (3) imaging radiation, were explored in multiple studies with consistent directionality of results. A total of 30 studies were observational, and 22 studies compared community hospital quality outcomes with other hospital types. The remaining 14 studies reported testing of interventions; 12 showed improved quality of care postintervention. All studies reported an outcome addressing safety, effectiveness, or efficiency, whereas timeliness, patient-centeredness, and equity were infrequently addressed. Risk of bias was moderate or high for 72% of studies.
CONCLUSIONS: Literature on the inpatient care of children in community hospitals is limited, making it difficult to evaluate healthcare quality. Measures of timeliness, patient-centeredness, and equity are underrepresented. The field would benefit from more multicenter collaborations to facilitate the application of robust study designs and to enable a systematic assessment of individual interventions and community hospital quality outcomes.
© 2019 Society of Hospital Medicine
Independent authors performed handsearches of Academic Pediatrics, BMJ Quality & Safety, Hospital Pediatrics, JAMA Pediatrics, and Pediatrics Quality Reports for the five years preceding the search date (July 2011-October 2016).
Study Selection and Definitions
To identify studies conducted in community hospitals, we operationalized the definition of community hospital proposed by Percelay.8 We used “community”, “general”, “nonuniversity”, and “nonchildren’s” as search terms and operationalized these through the addition of qualifying descriptors (Table 1).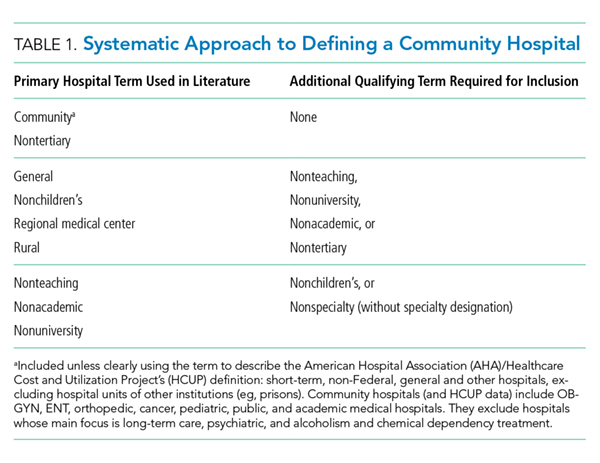
Studies were excluded if they (1) were performed outside of the United States, as community hospital definitions may differ by country; (2) included participants aged >18 years and did not report any pediatric-specific results; (3) were performed exclusively in tertiary hospitals; (4) evaluated only outpatient or emergency department care; (5) did not report any results specific to community hospitals; (6) did not report any data-driven or parent/patient-reported measures of safety, effectiveness, efficiency, timeliness, patient-centeredness, or equity in their results; and (7) were case reports, case series, editorials, or abstracts without an associated full-text article. We read commentaries and literature reviews related to our objectives and reviewed their references to identify additional articles, but did not include these manuscripts.
Two authors independently reviewed each abstract, and full-text articles were reviewed if one or more authors determined that the abstract met the inclusion criteria. Two authors then independently reviewed each full-text article to determine whether the article met the criteria for the final review. Disagreements were resolved through consensus after discussion and review with the entire research team, and reasons for exclusion were recorded.
Charting the Results and Data Synthesis
We used a standardized charting form to collect information regarding study design, community hospital terms, population descriptors, IOM aims of quality healthcare, and outcome measures. To minimize bias in data collection, information from each full-text article was extracted independently by two authors, and differences in extraction were resolved through discussion and re-review among the same two authors. To evaluate the quality of included evidence, two authors (JCL and JKL) independently assessed the risk of bias for each study using modified Newcastle-Ottawa Quality Assessment Scales (NOS), with disagreements resolved through discussion and re-review among the same two authors. For cohort studies, five of the eight NOS domains were relevant and applied to all included studies (maximum score 6). Using the NOS adapted for cross-sectional studies, six of the seven domains were relevant and applied (maximum score 9). For cross-sectional studies, we defined the risk of bias to be low for scores ≥8, moderate for scores 5-7, and high for scores ≤4, consistent with previous work.12 For cohort studies, we similarly defined these strata by scores ≥5, 3-4, and ≤2, given the lower maximum score for this study type.
We categorized studies as either observational, defined as cohort or cross-sectional studies of usual healthcare delivery, or interventional, defined as studies evaluating the development and/or implementation of an intervention designed to improve healthcare quality. We further categorized the studies into the following four overarching medical domains: (1) neonatal, (2) pediatric medicine, (3) surgery, or (4) radiology.
