Barriers to Providing VTE Chemoprophylaxis to Hospitalized Patients: A Nursing-Focused Qualitative Evaluation





BACKGROUND: Venous thromboembolism (VTE) is a serious medical condition that results in preventable morbidity and mortality.
OBJECTIVES: The objective of this study was to identify nursing-related barriers to administration of VTE chemoprophylaxis to hospitalized patients.
DESIGN: This was a qualitative study including nurses from five inpatient units at one hospital.
METHODS: Observations were conducted on five units to gain insight into the process for administering chemoprophylaxis. Focus group interviews were conducted with nurses and were audio-recorded, transcribed verbatim, and analyzed using the Theoretical Domains Framework to identify barriers to providing VTE chemoprophylaxis.
RESULTS: We conducted 14 focus group interviews with nurses from five inpatient units to assess nurses’ perceptions of barriers to administration of VTE chemoprophylaxis. The barriers identified included nurses’ misconceptions that ambulating patients did not require chemoprophylaxis, nurses’ uncertainty when counseling patients on the importance of chemoprophylaxis, and a lack of comparative data for nurses regarding their specific refusal rates.
CONCLUSIONS: Multiple factors act as barriers to patients receiving VTE chemoprophylaxis. These barriers are often modifiable targets for quality improvement. There is a need to focus on behavior changes that will remove or minimize barriers and equip nurses to ensure administration of VTE chemoprophylaxis by engaging patients in their care.
© 2019 Society of Hospital Medicine
Coding and Data Analysis
To develop the code book, the study team, consisting of three qualitative researchers, independently read one focus group transcript and applied the TDF domains to the nurses’ perceptions of barriers to administration of VTE chemoprophylaxis.21-24 In addition to coding by domain, the study team also coded nursing perceptions as barriers or facilitators. The study team reviewed the coded transcript and reconciled any differences in coding. This process was repeated for a second transcript, and then all remaining transcripts were assigned to two out of three study team members for coding, with the entire study team meeting to reconcile any differences. If necessary, the team member who did not code a transcript acted as the tie-breaker if there were discrepancies in codes that could not be reconciled.
Once coding was completed, we identified the TDF domains that were most relevant to the administration of VTE chemoprophylaxis.16 Member checking (testing the analysis, interpretations, and conclusions with members of those groups from whom the data were originally obtained) was performed with the four clinical nursing coordinators and four nurse managers from the participating units to establish face validity of the themes identified from the focus group interviews.25
The study team used MaxQDA, V12 (Berlin, Germany) to support data coding and analysis.26 The Northwestern University institutional review board office deemed this project research on nonhuman-subjects because it focused on the process of providing VTE chemoprophylaxis and not about the patients themselves. The purpose of the study was explained at the beginning of each focus group, and nurses gave verbal consent to have the focus group recorded.
RESULTS
We conducted 14 focus groups with day and night shift nurses from five units (two medical and three surgical) at a single institution. All nurses invited to participate in a focus group agreed to participate. The data were coded and grouped by domain and identified as barriers or facilitators. The findings included below are for the domains most relevant to the provision of VTE prophylaxis. Table 2 provides illustrative verbatim quotes for each domain that was represented in the focus groups.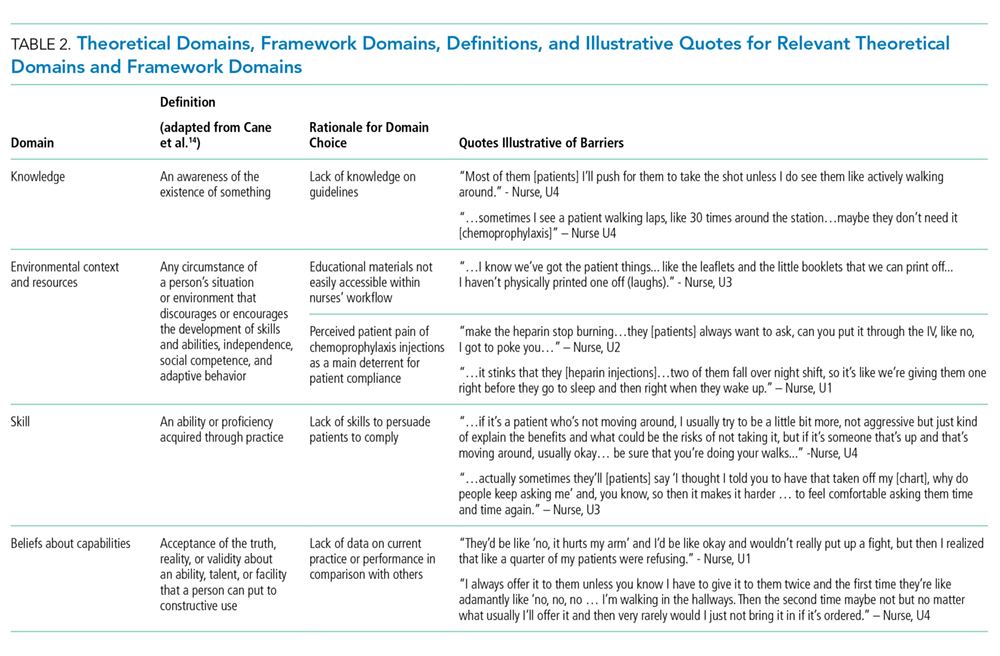
THEORETICAL DOMAINS FRAMEWORK DOMAINS
Knowledge
All interviewees recognized that providing some form of prophylaxis to mitigate the risk of a VTE event is essential. Some nurses stated that seeing a patient ambulating meant they would consider not administering prescribed chemoprophylaxis, while others would try to negotiate with patients by asking the patient to allow one dose of chemoprophylaxis prescribed two to three times daily because it was better than receiving no doses.
Environmental Context and Resources
Multiple barriers to providing optimal care were associated with the environmental context and a lack of resources. There was a lack of accessible, comprehensive, patient-centered education materials on VTE chemoprophylaxis to supplement a nurse’s explanation about the importance of chemoprophylaxis. Furthermore, many nurses cited the perceived patient pain of chemoprophylaxis injections as the main deterrent to patient compliance, especially subcutaneous heparin injections, which occur up to three times in 24 hours and often cause more pain at the site of injection than low-molecular-weight heparin. Nurses felt that transitioning patients from receiving subcutaneous heparin injections to receiving low-molecular-weight heparin could be a main driver to reduce patient refusals.
