Leveraging the Outpatient Pharmacy to Reduce Medication Waste in Pediatric Asthma Hospitalizations





BACKGROUND AND OBJECTIVE: Previous local quality improvement focused on discharging patients with inhaled corticosteroids (ICS) “in-hand” decreased healthcare reutilization after hospitalization for an asthma exacerbation. However, as a result of these new processes, some patients admitted for an asthma exacerbation received more than one ICS inhaler during their admission, contributing to medication waste and potential patient confusion regarding their discharge medication regimen. We sought to decrease this waste.
METHODS: We conducted a quality improvement project to reduce the prescribing of multiple ICS inhalers to patients at a large academic children’s hospital. Our primary outcome measure was the monthly percentage of patients admitted with an asthma exacerbation who were administered more than one ICS inhaler. A secondary outcome measure evaluated the reliability of the new process of using the hospital-based outpatient pharmacy to supply ICS “in-hand” and verify insurance coverage. After the process map review, we hypothesized a delay in the initial ICS treatment decision would allow for both a finalized discharge medication plan and a standardized process to verify outpatient insurance coverage. |
RESULTS: The mean percentage of patients receiving more than one ICS inhaler decreased from our baseline of 7.4% to 0.7%. Verification of outpatient prescription insurance coverage via the outpatient pharmacy increased from 0.7% to 50%. The average inpatient cost (average wholesale price) for ICS decreased by 62% to $90.25.
CONCLUSIONS: Our process change to use the outpatient pharmacy to dispense and verify insurance coverage for ICS medication was associated with a reduction in medication waste during admission for an asthma exacerbation.
© 2020 Society of Hospital Medicine
Measures
Our primary outcome measure was defined as the monthly number of patients admitted to Hospital Medicine for an acute asthma exacerbation administered more than one ICS divided by the total number of asthma patients administered at least one dose of an ICS (patient-supplied or dispensed from the inpatient pharmacy). A full list of ICS is included in the appendix Table.
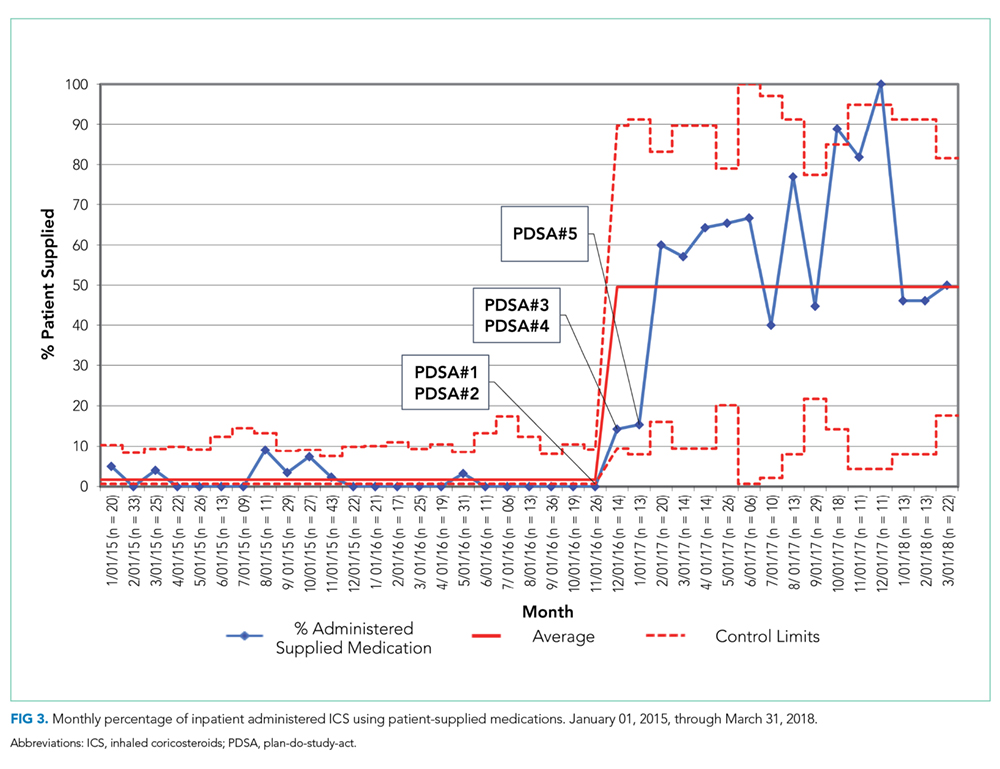
A secondary process measure approximated our adherence to obtaining ICS from the outpatient pharmacy for inpatient use. All medications administered during hospitalization are documented in the medication administration report. However, only medications dispensed from the inpatient pharmacy are associated with a patient charge. Patient-supplied medications, including those dispensed from the hospital outpatient pharmacy, are not associated with an inpatient charge. Therefore, the secondary process measure was defined as the monthly number of asthma patients administered an ICS not associated with an inpatient charge divided by the total number of asthma patients administered an ICS.
A cost outcome measure was developed to track changes in the average cost of an ICS included on inpatient bills during hospitalization for an asthma exacerbation. This outcome measure was defined as the total monthly cost, using the average wholesale price, of the ICS included on the inpatient bill for an asthma exacerbation, divided by the total number of asthma patients administered at least one dose of an ICS (patient supplied or dispensed from the inpatient pharmacy).
Our a priori intent was to reduce ICS medication waste while maintaining a highly reliable system that included inpatient administration and education with ICS devices and maintain our medications-in-hand practice. A balancing measure was developed to monitor the reliability of inpatient administration of ICS. It was defined as the monthly number of patients who received a discharge prescription for an ICS and were administered an ICS while an inpatient divided by the total number of asthma patients with a discharge prescription for an ICS.
Analysis
Measures were evaluated using statistical process control charts and special cause variation was determined by previously established rules. Our primary, secondary, and balancing measures were all evaluated using a p-chart with variable subgroup size. The cost outcome measure was evaluated using an X-bar S control chart.11-13
RESULTS
Primary Outcome Measure
During the baseline period, 7.4% of patients admitted to Hospital Medicine for an acute asthma exacerbation were administered more than one ICS, ranging from 0%-20% of patients per month (Figure 2). Following the start of our interventions, we met criteria for special cause allowing adjustment of the centerline.13 The mean percentage of patients receiving more than one ICS decreased from 7.4% to 0.7%. Figure 2 includes the n-value displayed each month and represents all patients admitted to the Hospital Medicine service with an asthma exacerbation who were administered at least one ICS.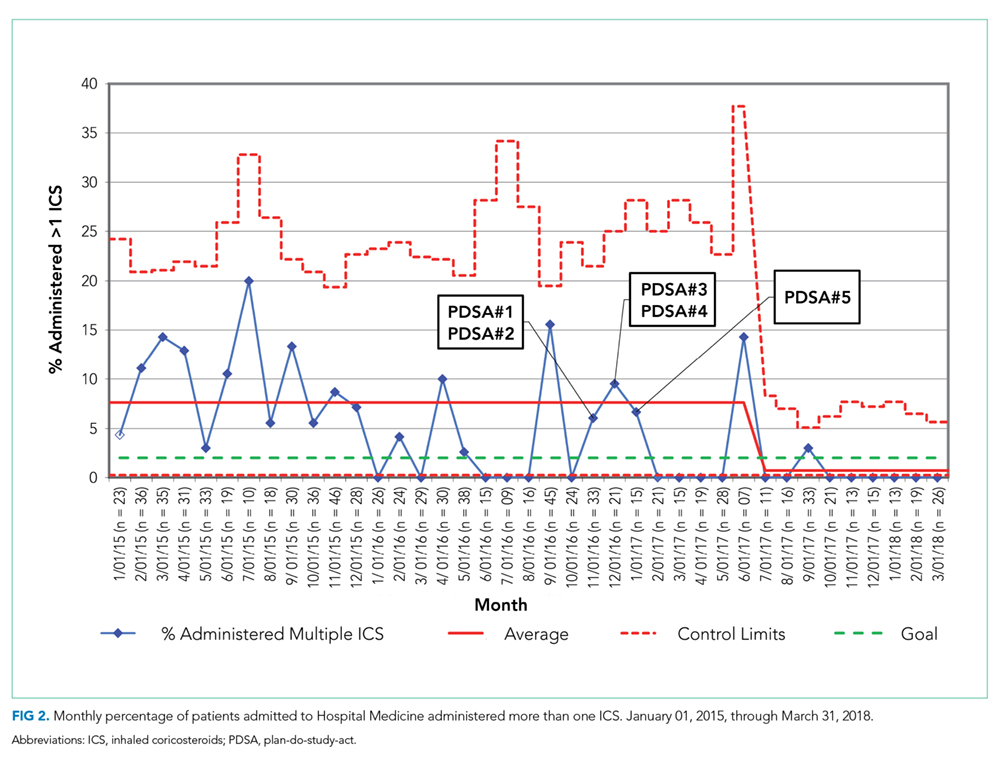
Secondary Process Measure
During the baseline period, there were only rare occurrences (less than 1%) of a patient-supplied ICS being administered during an asthma admission. Following the start of our intervention period, the frequency of inpatient administration of patient-supplied ICS showed a rapid increase and met rules for special cause with an increase in the mean percent from 0.7% to 50% (Figure 3). The n-value displayed each month represents all patients admitted to the Hospital Medicine service for an asthma exacerbation administered at least one ICS.