Discharge Medical Complexity, Change in Medical Complexity and Pediatric 30-day Readmission





BACKGROUND: While medical complexity is associated with pediatric readmission risk, less is known about how increases in medical complexity during hospitalization affect readmission risk.
METHODS: We conducted a five-year retrospective, case-control study of pediatric hospitalizations at a tertiary care children’s hospital. Cases with a 30-day unplanned readmission were matched to controls based on admission seasonality and distance from the hospital. Complexity variables included the number of medications prescribed at discharge, medical technology, and the need for home healthcare services. Change in medical complexity variables included new complex chronic conditions and new medical technology. We estimated odds of 30-day unplanned readmission using adjusted conditional logistic regression.
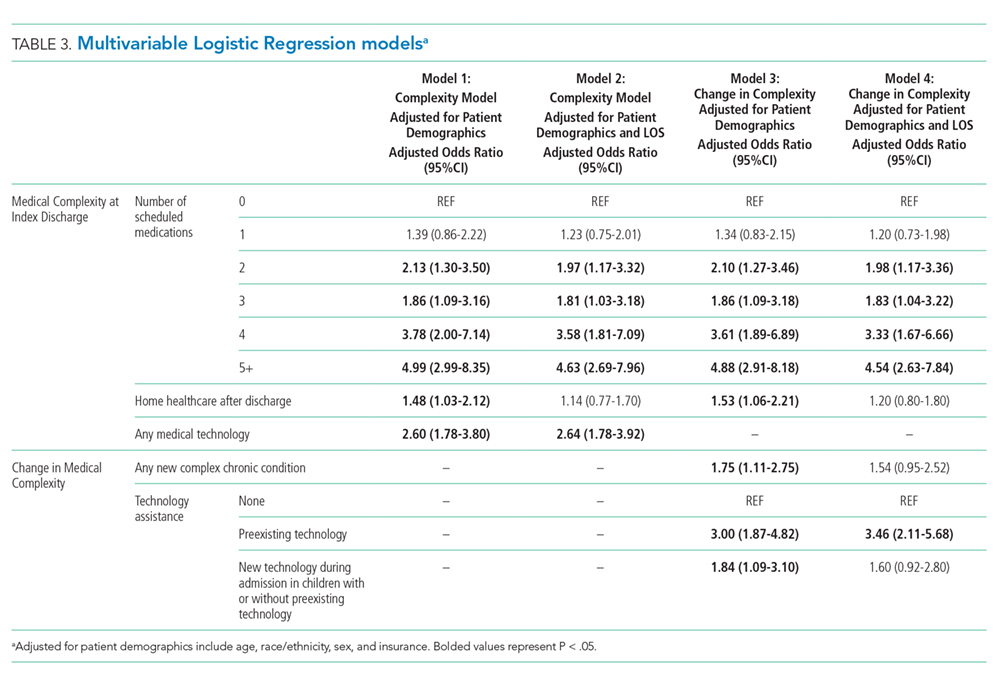
RESULTS: Of 41,422 eligible index hospitalizations, we included 595 case and 595 control hospitalizations. Complexity: Polypharmacy after discharge was common. In adjusted analyses, being discharged with ≥2 medications was associated with higher odds of readmission compared with being discharged without medication; children with ≥5 discharge medications had a greater than four-fold higher odds of readmission. Children assisted by technology had higher odds of readmission compared with children without technology assistance. Change in complexity: New diagnosis of a complex chronic condition (Adjusted Odds Ratio (AOR) = 1.75; 1.11-2.75) and new technology (AOR = 1.84; 1.09-3.10) were associated with higher risk of readmission when adjusting for patient characteristics. However, these associations were not statistically significant when adjusting for length of stay.
CONCLUSION: Polypharmacy and use of technology at discharge pose a substantial readmission risk for children. However, added technology and new complex chronic conditions do not increase risk when accounting for length of stay.
© 2019 Society of Hospital Medicine
DISCUSSION
We examined multiple attributes of polypharmacy—the number of scheduled medications, number of as-needed medications, and number of scheduled doses per 24 hours. Interestingly, only the scheduled medications (count of medication and number of doses) were associated with elevated readmission risk. As-needed medications have heterogeneity in the level of importance from critical (eg, seizure rescue) to discretionary (eg, antipyretics, creams). The burden of managing these types of medications may still be high (ie, parents must decide when to administer a critical medication); however, this burden does not translate into increased readmission risk in this population.
Not surprisingly, greater medical complexity—as defined by higher numbers of scheduled discharge medications and technology assistance—is associated with 30-day readmission risk. Our analyses do not allow us to determine how much of the increased risk is due to additional care burden and risks of polypharmacy versus the inherent increase in complexity and severity of illness for which polypharmacy is a marker. Tailoring discharge regimens to the realities of daily life, with the goal of “minimally disruptive medicine”22,23 (eg, integrating manageable discharge medication routines into school and work schedules), is not a common feature of pediatric discharge planning. For adult patients with complex medical conditions, tailoring medication regimens in a minimally disruptive way is known to improve outcomes.24 Similarly, adopting minimally disruptive techniques to integrate the polypharmacy inherent in discharge could potentially mitigate some of the readmission risks for children and adolescents.
Contrary to our hypothesis, new technologies and new diagnoses did not confer additional readmission risk when accounting for LOS and patient characteristics. One potential explanation is varying risks conveyed by different types of new technologies placed during hospitalization. Central lines, the most common form of new technology, is associated with higher odds of reutilization in unadjusted analyses. However, the second most common form of new technology, nonsurgically placed enteral feeding tube, was not. Further analyses of the differential effects of new technology should be further examined in larger datasets. Additionally, the lack of additional readmission risk from new technology may relate to additional teaching and support provided to families of patients undergoing unfamiliar procedures offsets the risks inherent of greater complexity. If so, it may be that the more intensive teaching and postdischarge support provided to families with new technology or a new diagnosis could be replicated through refresher teaching during hospitalizations, when a patient’s state of health is status quo for the family (ie, the child was admitted and discharged with the same technology and diagnoses). This notion is supported by prior work that demonstrated successful readmission reduction interventions for children with chronic conditions often rely on enhanced education or coaching.25,26
We elected to present models both with and without LOS as a confounder because it is a potentially modifiable attribute of hospitalization. Change in medical complexity aspects were significantly associated with readmission in multivariable models without LOS. However, with the addition of LOS, they were no longer significant. Thus, the readmission risk of new complexity is accounted for by the readmission risk inherent in a longer LOS. This finding prompts additional questions that merit further study: is it that LOS is a general marker for heightened complexity, or is it that a longer LOS can modify readmission risk through additional in-hospital care and time for enhanced education?
Our study has several strengths. We were able to discern true complexity at the time of discharge through medical record review. For example, if a child had a peripherally inserted central catheter placed during hospitalization, it cannot be ascertained through administrative data without medical record review if the technology was removed or in place at discharge. Likewise, medical record review allows for identification of medical technology which is not surgically implanted (eg, nasogastric feeding tubes). Given the “fog” families report as part of their in-hospital experience and its threats to education and postdischarge contingency planning,17 we felt it important to evaluate medical technology regardless of whether or not it was surgically placed. Additionally, the more detailed and nuanced understanding gained of polypharmacy burden can better inform both risk prediction models and interventions to improve the transition from hospital to home.
This study
