Collaboration, Not Calculation: A Qualitative Study of How Hospital Executives Value Hospital Medicine Groups





BACKGROUND: Hospital medicine groups (HMGs) typically receive financial support from hospitals. Determining a fair amount of financial support requires negotiation between HMG and hospital leaders. As the hospital medicine care model evolves, hospital leaders may regularly challenge HMGs to demonstrate the financial value of activities that do not directly generate revenue.
OBJECTIVE: To describe current attitudes and beliefs of hospital executives regarding the value of contributions made by HMGs. DESIGN: Thematic content analysis of key informant interviews.
PARTICIPANTS: Twenty-four healthcare institutional leaders, including hospital presidents, chief medical officers, chief executive officers, and chief financial officers. Participants comprised a diverse sample from all regions in the United States, including rural, suburban, and urban locations, and academic and nonacademic institutions.
RESULTS: Executives highly valued hospitalist groups that demonstrate alignment with hospital priorities, and often used this concept to summarize the HMG’s success across several value domains. Most executives evaluated only a few key HMG metrics, but almost no executives reported calculating the HMG return on investment by summing pertinent quantitative contributions. Respondents described an evolving concept of hospitalist value and believed that HMGs generate substantial value that is difficult to measure financially.
CONCLUSIONS: Hospital executives appear to make financial support decisions based on a small number of basic financial or care quality metrics combined with a subjective assessment of the HMG’s broader alignment with hospital priorities. HMG leaders should focus on building relationships that facilitate dialog about alignment with hospital needs.
© 2019 Society of Hospital Medicine
The general absence of summary value calculations suggests specific opportunities, benefits, and risks for HMG group leaders (Table 3). An important opportunity relates to the communication agenda about unmeasured or nonfinancial contributions. Although executives recognized many of these, our data suggest a need for HMG leaders to educate hospital leaders about their unmeasured contributions proactively. Although some might recommend doing so by quantifying and financially rewarding key intangible contributions (eg, measuring leadership in culture change9), this entails important risks.10 Some experts propose that the proliferation of physician pay-for-performance schemes threatens medical professionalism, fails patients, and misunderstands what motivates physicians.11 HMG groups that feel undervalued should hesitate before monetizing all aspects of their work, and consider emphasizing relationship-building as a platform for communication about their performance. Achieving better alignment with executives is not just an opportunity for HMG leaders, but for each hospitalist within the group. Although executives wanted to have deeper relationships with group members, this may not be feasible in large organizations. Instead, it is incumbent for HMG leaders to translate executives’ expectations and forge better alignment.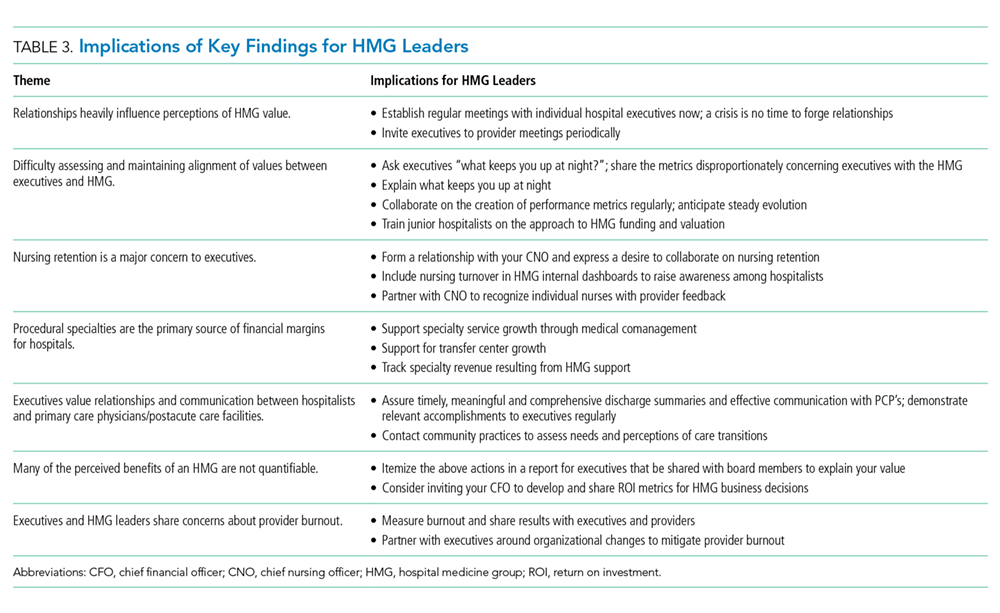
Residency may not adequately prepare hospitalists to meet key expectations hospital executives hold related to system leadership and interprofessional team leadership. For example, hospital leaders particularly valued HMGs’ perceived ability to improve nurse retention and morale. Unfortunately, residency curricula generally lack concerted instruction on the skills required to produce such interprofessional inpatient teams reliably. Similarly, executives strongly wanted HMGs to acknowledge a role as partners in running the quality, stewardship, and safety missions of the entire hospital. While residency training builds clinical competence through the care of individual patients, many residents do not receive experiential education in system design and leadership. This suggests a need for HMGs to provide early career training or mentorship in quality improvement and interprofessional teamwork. Executives and HMG leaders seeking a stable, mature workforce, should allocate resources to retaining mid and late career hospitalists through leadership roles or financial incentives for longevity.
As with many qualitative studies, the generalizability of our findings may be limited, particularly outside the US healthcare system. We invited executives from diverse practice settings but may not have captured all the relevant viewpoints. This study did not include Veterans Affairs hospitals, safety net hospitals were underrepresented, Midwestern hospitals were overrepresented and the participants were predominantly male. We were unable to determine the influence of employment model on participant beliefs about HMGs, nor did we elicit comparisons to other physician specialties that would highlight a distinct approach to negotiating with HMGs. Because we used hospitalists as interviewers, including some from the same institution as the interviewee, respondents may have dampened critiques or descriptions of unmet expectations. Our data do not provide quantitative support for any approach to determining or negotiating appropriate financial support for an HMG.
CONCLUSIONS
This work contributes new understanding of the expectations executives have for HMGs and individual hospitalists. This highlights opportunities for group leaders, hospitalists, medical educators, and quality improvement experts to produce a hospitalist labor force that can engage in productive and mutually satisfying relationships with hospital leaders. Hospitalists should strive to improve alignment and communication with executive groups.
