Improving Respiratory Rate Accuracy in the Hospital: A Quality Improvement Initiative





Respiratory rate (RR) is a predictor of adverse outcomes. However, RRs are inaccurately measured in the hospital. We conducted a quality improvement (QI) initiative using plan-do-study-act methodology on one inpatient unit of a safety-net hospital to improve RR accuracy. We added time-keeping devices to vital sign carts and retrained patient-care assistants on a newly modified workflow that included concomitant RR measurement during automated blood pressure measurement. The median RR was 18 (interquartile range [IQR] 18-20) preintervention versus 14 (IQR 15-20) postintervention. RR accuracy, defined as ±2 breaths of gold-standard measurements, increased from 36% preintervention to 58% postintervention (P < .01). The median time for vital signs decreased from 2:36 minutes (IQR, 2:04-3:20) to 1:55 minutes (IQR, 1:40-2:22; P < .01). The intervention was associated with a 7.8% reduced incidence of tachypnea-specific systemic inflammatory response syndrome (SIRS = 2 points with RR > 20; 95% CI, –13.5% to –2.2%). Our interdisciplinary, low-cost, low-tech QI initiative improved the accuracy and efficiency of RR measurement.
© 2019 Society of Hospital Medicine
Respiratory rate (RR) is an essential vital sign that is routinely measured for hospitalized adults. It is a strong predictor of adverse events.1,2 Therefore, RR is a key component of several widely used risk prediction scores, including the systemic inflammatory response syndrome (SIRS).3
Despite its clinical utility, RR is inaccurately measured.4-7 One reason for the inaccurate measurement of RR is that RR measurement, in contrast to that of other vital signs, is not automated. The gold-standard technique for measuring RR is the visual assessment of a resting patient. Thus, RR measurement is perceived as time-consuming. Clinical staff instead frequently approximate RR through brief observation.8-11
Given its clinical importance and widespread inaccuracy, we conducted a quality improvement (QI) initiative to improve RR accuracy.
METHODS
Design and Setting
We conducted an interdisciplinary QI initiative by using the plan–do–study–act (PDSA) methodology from July 2017 to February 2018. The initiative was set in a single adult 28-bed medical inpatient unit of a large, urban, safety-net hospital consisting of general internal medicine and hematology/oncology patients. Routine vital sign measurements on this unit occur at four- or six-hour intervals per physician orders and are performed by patient-care assistants (PCAs) who are nonregistered nursing support staff. PCAs use a vital signs cart equipped with automated tools to measure vital signs except for RR, which is manually assessed. PCAs are trained on vital sign measurements during a two-day onboarding orientation and four to six weeks of on-the-job training by experienced PCAs. PCAs are directly supervised by nursing operations managers. Formal continuing education programs for PCAs or performance audits of their clinical duties did not exist prior to our QI initiative.
Intervention
Intervention development addressing several important barriers and workflow inefficiencies was based on the direct observation of PCA workflow and information gathering by engaging stakeholders, including PCAs, nursing operations management, nursing leadership, and hospital administration (PDSA cycles 1-7 in Table). Our modified PCA vital sign workflow incorporated RR measurement during the approximate 30 seconds needed to complete automated blood pressure measurement as previously described.12 Nursing administration purchased three stopwatches (each $5 US) to attach to vital signs carts. One investigator (NK) participated in two monthly one-hour meetings, and three investigators (NK, KB, and SD) participated in 19 daily 15-minute huddles to conduct stakeholder engagement and educate and retrain PCAs on proper technique (total of 6.75 hours).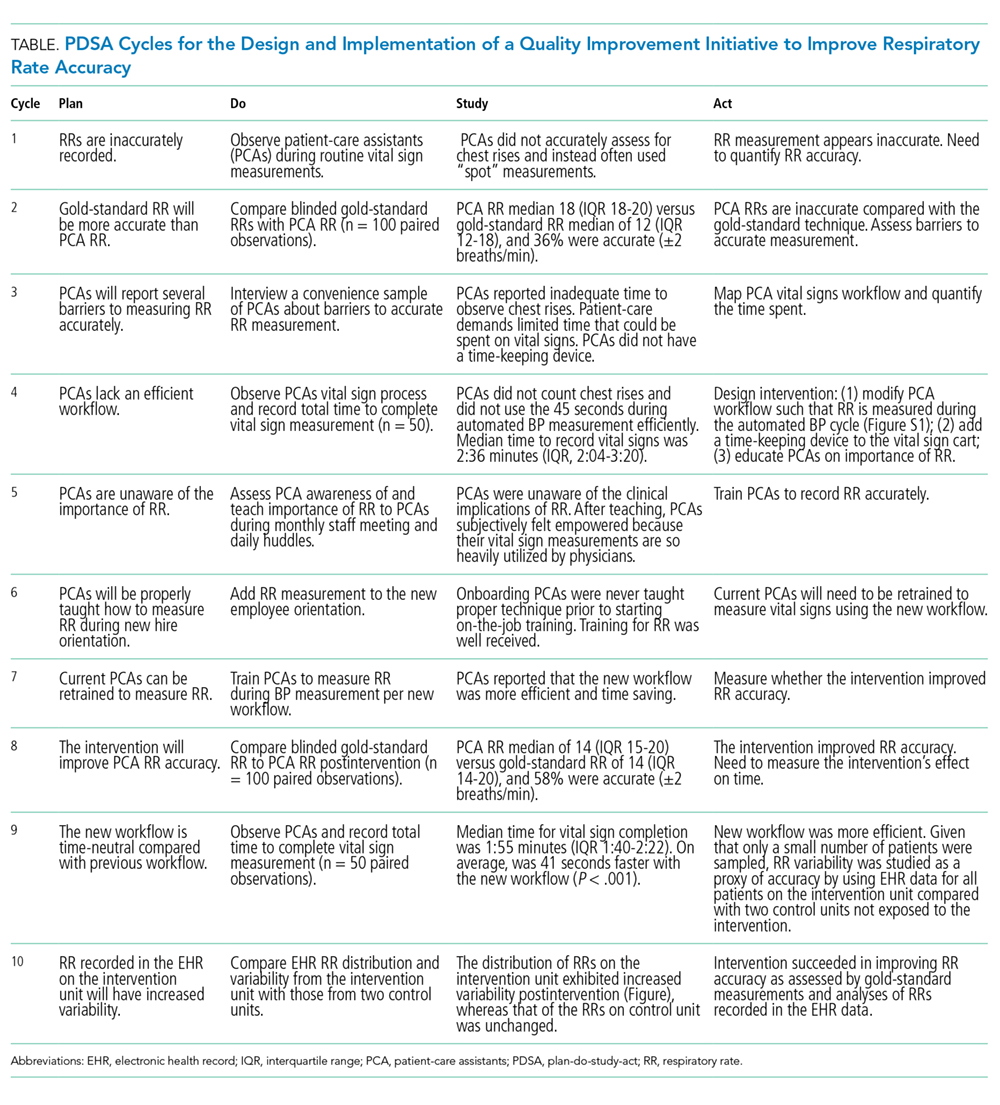
Evaluation
The primary aim of this QI initiative was to improve RR accuracy, which was evaluated using two distinct but complementary analyses: the prospective comparison of PCA-recorded RRs with gold-standard recorded RRs and the retrospective comparison of RRs recorded in electronic health records (EHR) on the intervention unit versus two control units. The secondary aims were to examine time to complete vital sign measurement and to assess whether the intervention was associated with a reduction in the incidence of SIRS specifically due to tachypnea.
