An Acute Care for Elders Quality Improvement Program for Complex, High-Cost Patients Yields Savings for the System





BACKGROUND: Acute Care for Elders (ACE) programs improve outcomes for older adults; however, little is known about whether impact varies with comorbidity severity.
OBJECTIVE: To describe differences in hospital-level outcomes between ACE and routine care across various levels of comorbidity burden.
DESIGN: Cross-sectional quality improvement study.
SETTING: A 716-bed teaching hospital.
PARTICIPANTS: Medical inpatients aged ≥70 years hospitalized between September 2014 and August 2017.
INTERVENTION: ACE care, including interprofessional rounds, geriatric syndromes screening, and care protocols, in an environment prepared for elders
MEASUREMENTS: Total cost, length of stay (LOS), and 30-day readmissions. We calculated median differences for cost and LOS between ACE and usual care and explored variations across the distribution of outcomes at the 25th, 50th, 75th and 90th percentiles. Results were also stratified across quartiles of the combined comorbidity score.
RESULTS: A total of 1,429 ACE and 10,159 non-ACE patients were included in this study. The mean age was 81 years, 57% were female, and 81% were white. ACE patients had lower costs associated with care ranging from $171 at the 25th percentile to $3,687 at the 90th percentile, as well as lower LOS ranging from 0 days at the 25th percentile to 1.9 days at the 90th percentile. After stratifying by comorbidity score, the greatest differences in outcomes were among those with higher scores. There was no difference in 30-day readmission between the groups.
CONCLUSION: The greatest reductions in cost and LOS were in patients with greater comorbidity scores. Risk stratification may help hospitals prioritize admissions to ACE units to maximize the impact of the more intensive intervention.
© 2019 Society of Hospital Medicine
Exposure
Subjects were categorized as either discharged from the ACE or discharged from usual care. ACE discharges were tracked daily on a spreadsheet that was linked into our sample of eligible subjects.
Outcomes
Total cost of hospitalization (direct plus indirect costs), LOS, and all-cause 30-day readmissions were queried from the same billing database.
Statistical Analysis
As this study was a quality improvement project, analyses were descriptive and exploratory; no statistical hypothesis testing was conducted. We initially evaluated subject characteristics and comorbidities across study groups to determine group balance and comparability using means and standard deviations for continuous data and frequencies and percentages for categorical data. To analyze total cost and LOS, we utilized quantile regression with clustered standard errors to account for clustering by patient. We calculated the median difference between hospitalization cost and LOS for usual care versus ACE patients (with ACE as the referent group). To explore variations across the distributions of outcomes, we determined differences in cost and LOS and their 95% confidence intervals at the 25th, 50th, 75th, and 90th percentiles. Thirty-day readmission risk was estimated using a generalized estimating equation model with a logit link and binomial family. Readmission risk is presented along with 95% confidence intervals. For all models, we initially evaluated change over time (by quarter). After establishing the absence of time trends, we collapsed results into a comparison of usual care versus ACE care. Model estimates are presented both unadjusted and adjusted for age and comorbidity score. Following our initial analyses of cost, LOS, and 30-day readmission risk; we explored differences across quartiles of combined comorbidity scores. We used the same unadjusted models described above but incorporated an interaction term to generate estimates stratified by quartile of comorbidity score. We performed two additional analyses to evaluate the robustness of our findings. First, because hemiplegia prevalence was higher in the usual-care group than in the ACE group and can result in higher cost of care, we repeated the analysis after excluding those patients with hemiplegia. Second, because we were unable to control for functional capacity in the entire sample, we evaluated group differences in mobility for a subsample obtained prior to October 2015 using ICD-9 diagnostic codes, which can be considered surrogate markers for mobility.22 The results of our first analysis did not substantively change our main findings; in our second analysis, groups were balanced by mobility factors which suggested that confounding by functional capacity would be limited in our full sample. The results of these analyses are reported in the supplemental material.
Analysis was completed using Stata v15.1 (StataCorp, LP College Station, Texas). The Baystate Medical Center Institutional Review Board determined that the initiative was quality improvement and “not research.”
RESULTS
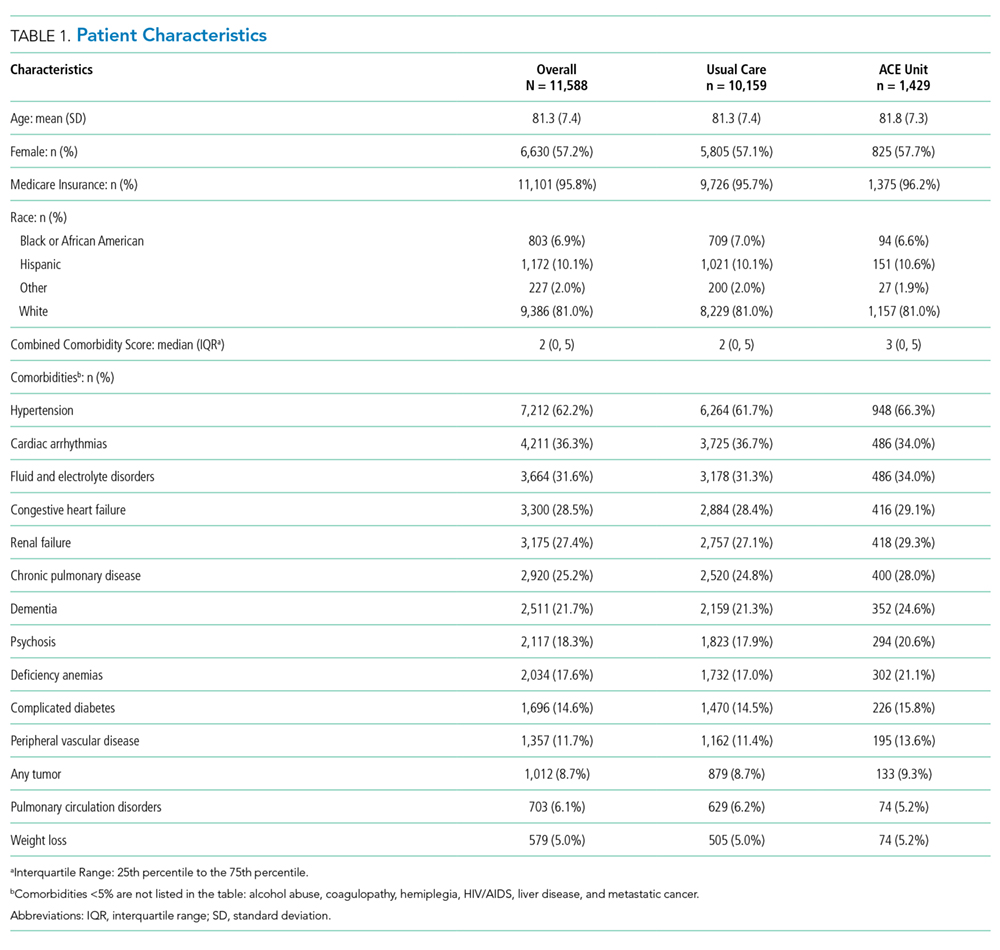
A total of 13,209 patients met the initial inclusion criteria; 1,621 were excluded, resulting in a sample of 11,588 patients. Over the 3-year study period, 1,429 (12.3%) were discharged from ACE and 10,159 (87.7%) were discharged from usual care. The groups were similar in age, sex, race and insurance status. Compared with the usual-care group, ACE patients had a higher median comorbidity score (3 vs 2 for usual care) and higher rates for anemia, dementia, fluid and electrolyte disorders, hypertension, and chronic obstructive pulmonary disease (COPD). However, ACE patients had lower rates of hemiplegia (0.9% vs 3%), arrhythmias, and pulmonary circulation disorders than those with usual care (Table 1).