Assess Before Rx: Reducing the Overtreatment of Asymptomatic Blood Pressure Elevation in the Inpatient Setting





BACKGROUND: Asymptomatic blood pressure elevation is common in the inpatient setting. National guidelines recommend treating with oral agents to slowly decrease blood pressure; however, many clinicians use intravenous antihypertensive medications, which can lead to unpredictable changes in blood pressure.
OBJECTIVE: To decrease the number of inappropriate orders (without symptoms of hypertensive emergency or order for NPO) of intravenous antihypertensives and adverse events associated with intravenous orders.
DESIGN: Quasi-experimental study with multidisciplinary intervention. PARTICIPANTS: Inpatients with a one-time order for an intravenous antihypertensive agent from January 2016 to February 2018.
MAIN MEASURES: The main outcomes were the total numbers of orders and inappropriate orders, adverse events, and alternate etiologies per 1,000 patient-days. As a balancing measure, patients were monitored for adverse events when blood pressure was elevated and not treated.
KEY RESULTS: There were a total of 260 one-time orders of intravenous antihypertensives on two medical units. Inappropriate orders decreased from 8.3 to 3.3 per 1,000 patient days (P = .0099). Adverse events associated with intravenous antihypertensives decreased from 3.7 to 0.8 per 1,000 patient days (P = .0072).
CONCLUSION: This initiative demonstrated a significant reduction in inappropriate use of IV antihypertensives and an associated reduction in adverse events.
© 2019 Society of Hospital Medicine
For this study, orders were reported on the standardized form of orders per 1,000 patient days. This was calculated as the number of orders divided by the total number of patient days from the two medicine units. For the univariate analysis, pre- and postintervention orders were compared for the different order categories using a t-test. Results were considered statistically significant at P < .05. Data analysis was conducted using SAS v. 9.4 (SAS Institute, Cary, North Carolina).
Additionally, a cost analysis was performed to estimate the hospital-wide annual cost of inappropriate orders. The analysis used the cost per dose12 and included nurse-time derived from the median salary of those on our units. The hospital-wide cost was extrapolated to estimate the potential annual savings for the institution.
RESULTS
A total of 260 one-time orders of IV antihypertensives were analyzed in this study, 127 in the seven-month preintervention period and 133 in the 12-month postintervention period. The majority, 67.3% (n = 175), were labetalol orders. Inappropriate orders (ie, neither NPO nor hypertensive emergency) decreased from 8.3 to 3.3 orders per 1,000 patient days (P = .0099; Figure 3).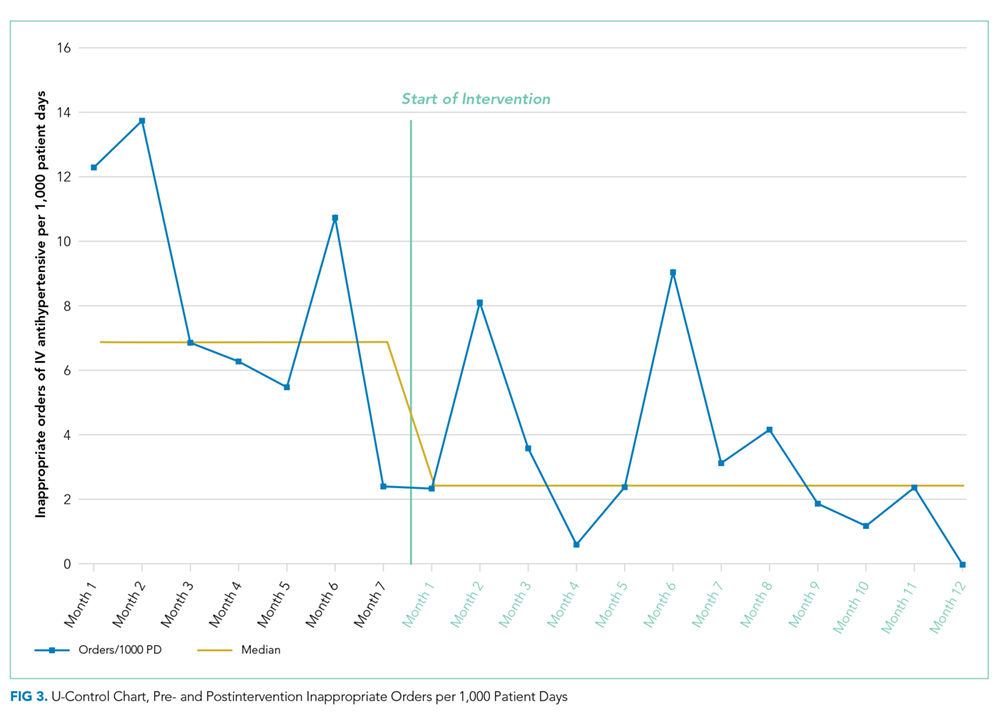
In total, there were 86 adverse events (33.1%), the majority of which (94.2%, n = 81) were a >25% decrease in blood pressure (Table 1). The number of adverse events per 1,000 patient days decreased from 4.4 in the preintervention period to 1.9 postintervention, P = .0112. Of the inappropriate orders, adverse events decreased from 3.7 to 0.8 per 1,000 patient days, P = .0072. Overall, there were 76 orders (29.2%) with documented alternate etiologies. The number of orders per 1,000 patient days with an alternate etiology decreased from 4.7 in the preintervention period to 1.2 postintervention, P =.0044 (Table 2). Descriptive analysis of patient characteristics pre-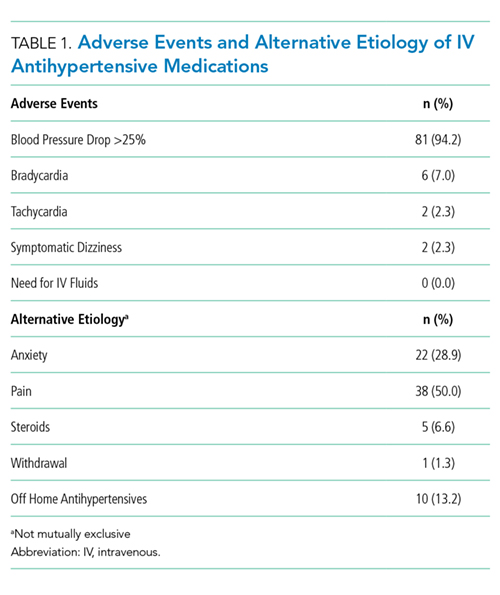
Cost analysis estimated a $17,890 annual hospital-wide cost for unnecessary IV antihypertensive medications before the intervention. The estimate was calculated using the number of orders on the two medical units observed during the seven-month preintervention period, extrapolated to a 12-month period and to the total number of 15 medical units in the hospital. The intervention on the two studied medical units themselves led to an estimated $1,421 cost reduction (59.6%). Had the intervention been implemented hospital-wide with similar results, the resulting cost reduction would have amounted to $10,662.
DISCUSSION
Our initiative successfully demonstrated a significant reduction of 60% in inappropriate one-time orders of IV antihypertensives per 1,000 patient days. Accordingly, the number of adverse events per 1,000 patient days decreased by 57%. There was also a decrease in the number and percentage of IV orders with documented alternate etiologies. We hypothesize that this was due to nurses and physicians assessing and treating these conditions prior to treating hypertension in the intervention period, consequently avoiding an IV order.