Predicting the Future: Using Simulation Modeling to Forecast Patient Flow on General Medicine Units





BACKGROUND: Hospitals are complex adaptive systems within which multiple components such as patients, practitioners, facilities, and technology interact. A careful approach to optimization of this complex system is needed because any change can result in unexpected deleterious effects. One such approach is discrete event simulation, in which what-if scenarios allow researchers to predict the impact of a proposed change on the system. However, studies illustrating the application of simulation in optimization of general internal medicine (GIM) team inpatient operations are lacking.
METHODS: Administrative data about admissions and discharges, data from a time-motion study, and expert opinion on workflow were used to construct the simulation model. Then, the impact of four changes – aligning medical teams with nursing units, adding a hospitalist team, adding a nursing unit, and adding both a nursing unit and hospitalist team with higher admission volume – were modeled on key hospital operational metrics.
RESULTS: Aligning medical teams with nursing units improved team metrics for aligned teams but shifted patients to unaligned teams. Adding a hospitalist team had little benefit, but adding a nursing unit improved system metrics. Both adding a hospitalist team and a nursing unit would be required to maintain operational metrics with increased patient volume.
CONCLUSION: Using simulation modeling, we provided data on the implications of four possible strategic changes on GIM inpatient units, providers, and patient throughput. Such analyses may be a worthwhile investment to study strategic decisions and make better choices with fewer unintended consequences.
© 2019 Society of Hospital Medicine
For Future States 1-3, admission volume was held constant. The model generated nursing unit LOS using a random continuous exponential probability distribution with a mean of 133 hours to match the LOS distribution derived from health system data. As patients entered the system for admission, the model assigned a bed to the patient, but the patient could not move to the assigned bed until a bed and care team were both available. We were only interested in the steady-state behavior of the system, so collecting performance statistics only after the model had been populated and steady state had been achieved was important.
Table 1 summarizes the input data, fixed, and dynamic variable for each future state model.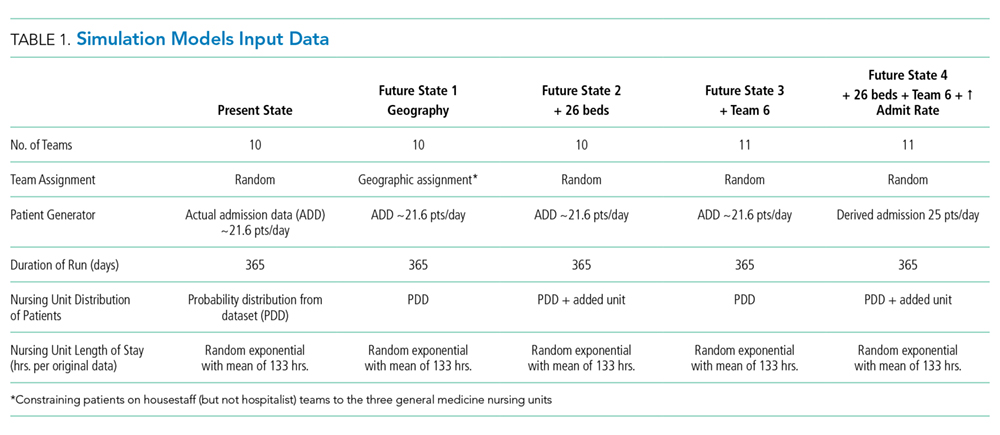
We examined the impact of these scenarios on the following variables (Table 2): (1) average time in system; (2) average number of patients waiting for a bed; (3) average ED boarding time; (4) total daily general medicine census; (5) average housestaff team census per team; (6) average hospitalist team census per team; (7) average combined housestaff and hospitalist team census per team; (8) average housestaff team utilization (ie, mean team census divided by team patient capacity of 16); (9) average hospitalist team utilization (ie, mean team census divided by team patient capacity of 16); (10) average nursing unit utilization (ie, mean nursing unit census divided by maximum number of patients that can be cared for on each nursing unit); (11) patient dispersion to NUs (ie, average number of NUs on which each general medicine team has patients); 12) estimated average rounding time per general medicine team.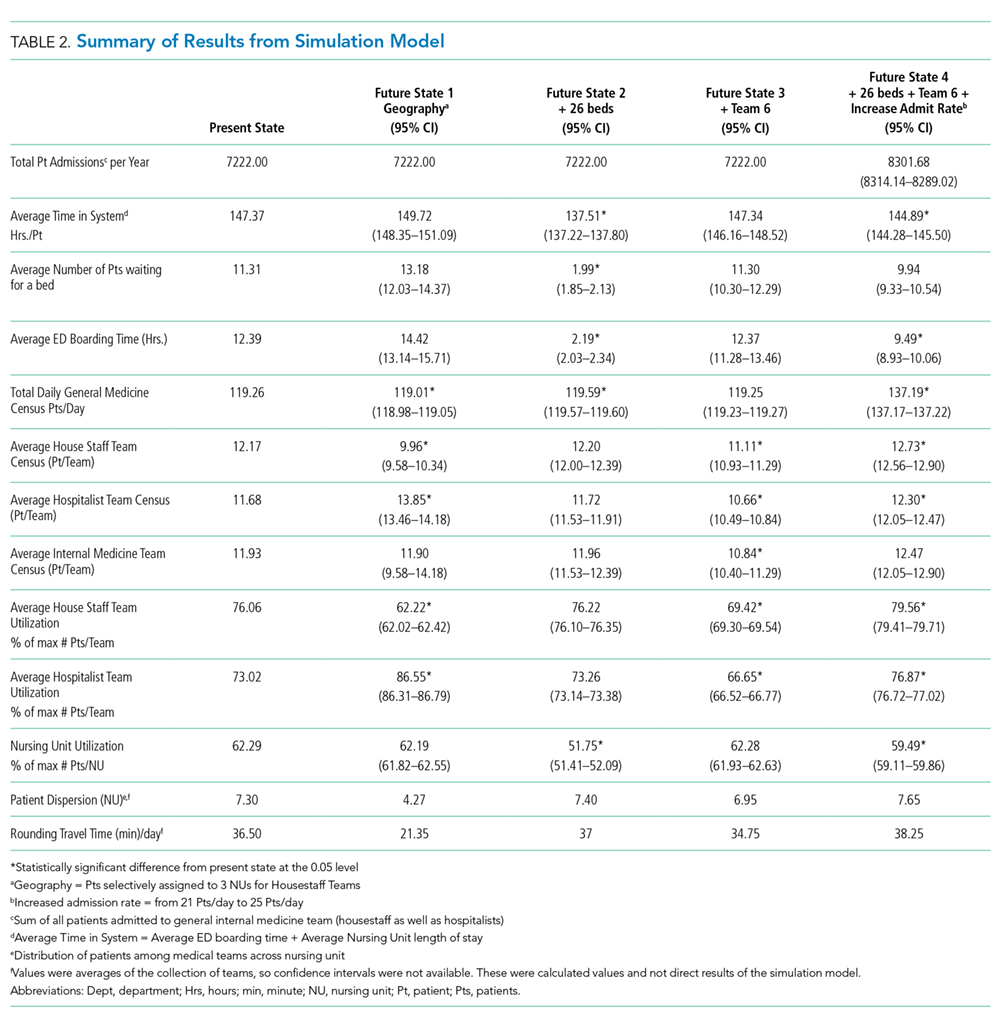
Of note, the average time in the system included time patients spent waiting for bed and team assignments (ED boarding time) in addition to the time they spent in the assigned nursing unit (nursing LOS). The difference between the nursing LOS (ie, time on the nursing unit) and total time in the system is one indicator of system efficiency around hospital admission.
The Institutional Review Board of Virginia Commonwealth University approved this study.
RESULTS
Time and Motion Data
The mean time spent with each patient was nine minutes. The mean time traveling between NUs Healthcare Quality for Children and Adolescents with Suicidality Admitted to Acute Care Hospitals in the United States was five minutes. Average rounding time was noted to be two hours, 53 minutes. Thirty-seven minutes, about ~21% of the time, was wasted in traveling. Each team, on average, traveled to seven different NUs to round on their daily census, averaging 1.6 patients in each nursing unit.
Hospital Data
Between January 1, 2011 to December 31, 2013, a total of 7,902 patients were admitted to the general medicine teams, spanning 23 NU. The average number of admissions per day was 21.6, and the average nursing unit LOS was 133 hours. Average team census was derived from historical data across all GIM team for 2013 and was noted to be 11.5 patients per team, and these patients were spread over seven NU.